THE NUMBERS ARE TOO BIG TO IGNORE
I am a big believer in numbers.
Why?
Because numbers scream, and people talk.
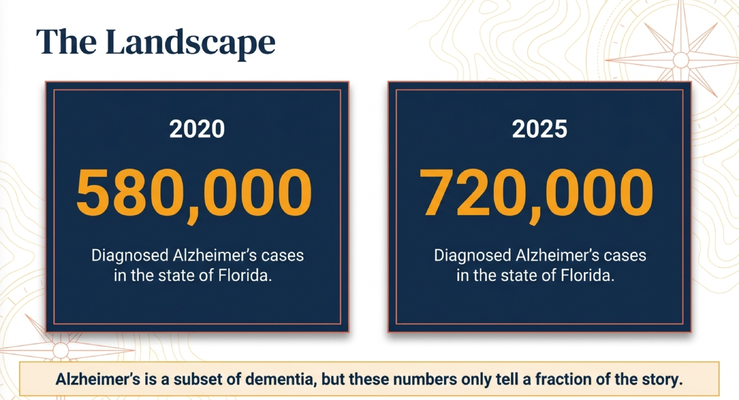
Here in Florida, the number of people diagnosed with Alzheimer’s disease was about 580,000 in 2020.
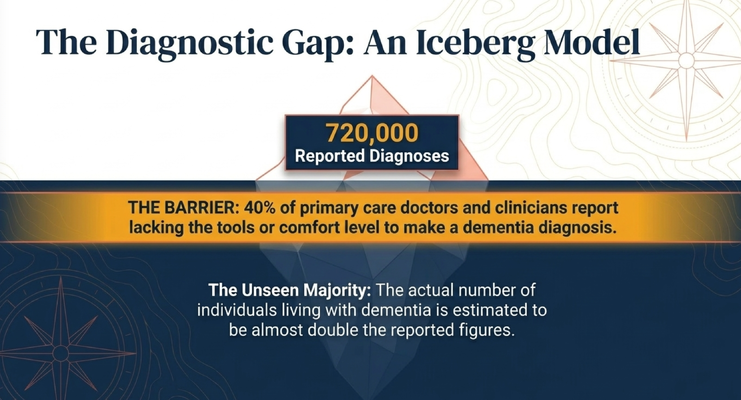
By 2025, that number was estimated at 720,000.
That is a major increase in a short period of time.
And remember, Alzheimer’s disease is only one type of dementia. It is a subset of dementia. So when we talk about Alzheimer’s disease numbers, we are not even talking about every person living with cognitive decline from every dementia type.
Now here is the other part that should make every family and professional pause.
Around 40% of primary care doctors and clinicians report that they either do not feel comfortable or do not feel they have the tools to make a dementia diagnosis.
So let’s think about that.
If 720,000 people in Florida are already diagnosed with Alzheimer’s disease, but a large portion of clinicians say they are uncomfortable making the diagnosis, then is that number fully accurate?
Probably not.
It may be on the low side.
And that means there may be many families living with dementia without a clear diagnosis, without staging, without planning, and without the support they need.
THE DIAGNOSTIC GAP
The diagnostic gap matters because families often wait too long.
A loved one starts repeating questions.
They miss appointments.
They become more forgetful.
They start struggling with bills.
They get lost while driving.
They become confused in situations that used to be simple.
And then the family may hear:
“It is probably just normal aging.”
“Let’s wait and see.”
“Come back if it gets worse.”
But dementia care cannot only be reactive.
Because by the time a family says, “Okay, this is really a problem,” the person may already be in the moderate stage. And once someone is moderate, certain treatment windows, planning windows, and decision-making windows may already be closing.
That is why early diagnosis matters.
Not because a blood test or a memory test magically solves everything.
But because early diagnosis gives families time.
Time to plan.
Time to understand.
Time to talk about driving.
Time to talk about finances.
Time to talk about power of attorney.
Time to talk about advance directives.
Time to talk about home safety.
Time to talk about support.
Time to ask the difficult questions before the family is trapped in a difficult situation.
THE “MAMMOGRAM MOMENT” FOR ALZHEIMER’S DISEASE
I recently came back from Washington, D.C. with the Alzheimer’s Association.
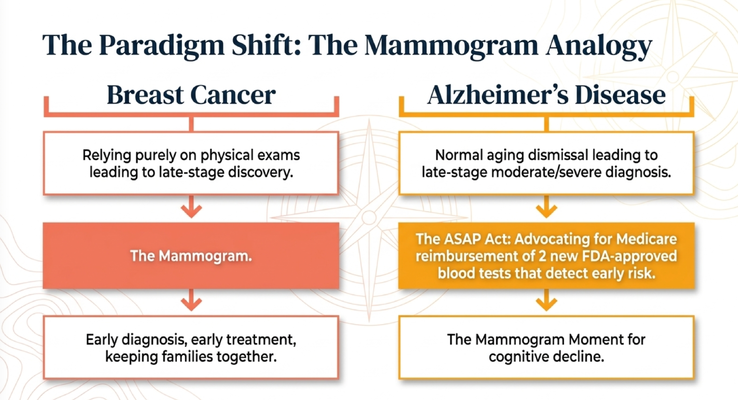
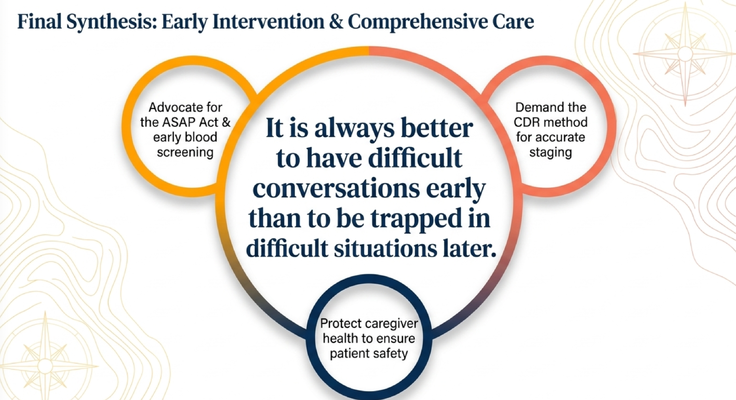
We were advocating for the ASAP Act — the Alzheimer’s Screening and Prevention Act.
And I want families to understand why this matters.
Think back to breast cancer screening.
Before mammograms became part of routine screening, many women were diagnosed later. Once screening became more available, the goal became earlier detection, earlier treatment, and better planning.
That is why I call this moment in Alzheimer’s disease our “mammogram moment.”
We now have emerging blood-based testing that may help identify Alzheimer’s-related biology earlier in the disease process. That does not mean every person should randomly test themselves. It does not replace a clinical evaluation. It does not replace the doctor, cognitive testing, functional assessment, imaging, medical history, or family observations.
But it may become part of a better pathway.
Because if someone is beginning to show memory changes, and the doctor says, “It might just be aging,” a better screening pathway could help families get clarity sooner.
And clarity matters.
Because there are newer treatment conversations that may only apply earlier in the disease. If someone is already moderate, certain options may no longer be appropriate.
So the timing is not a minor detail.
Timing can change what is possible.
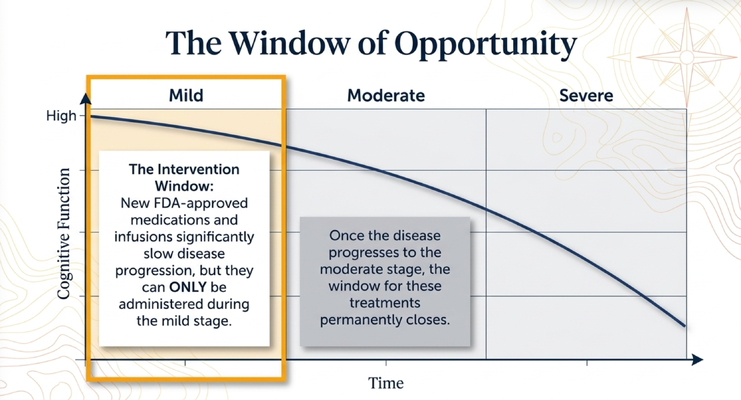
THE WINDOW OF OPPORTUNITY
This is one of the most important points I want caregivers to understand.
Dementia is progressive.
In many cases, especially Alzheimer’s disease, the disease unfolds slowly over years. But that does not mean every stage is the same.
Early stage is different from middle stage.
Middle stage is different from late stage.
And what you do in each stage matters.
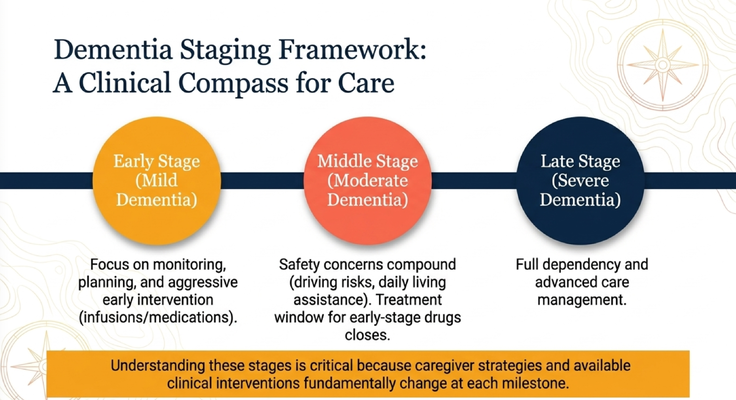
In the mild stage, the person may still be able to participate in decisions. They may still understand legal planning. They may still be able to discuss driving, finances, goals of care, home safety, and what kind of care they would want later.
In the moderate stage, safety concerns start compounding. Driving may become unsafe. Medication management may become unreliable. Showering may become difficult. Wandering risk may increase. The caregiver may need more support.
In the severe stage, the person may become fully dependent. Now the focus shifts toward comfort, safety, dignity, feeding, skin care, swallowing, infection risk, and advanced care planning.
This is why I always tell families:
It is better to have difficult conversations early than to be trapped in difficult situations later.
If you wait until the person cannot participate anymore, now the family is guessing.
What would Mom have wanted?
Who should make decisions?
Should Dad still be at home?
Would she have wanted intubation?
Would he have wanted CPR?
Who handles the finances?
Who is the healthcare proxy?
Those conversations are much harder when the disease has already progressed.
THE CAREGIVER IS PART OF THE DISEASE STORY
Now let’s talk about caregivers.
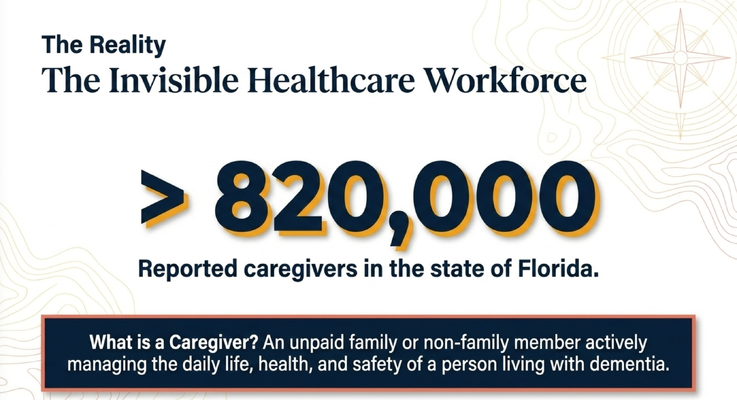
In Florida, there are more than 820,000 reported caregivers for people living with dementia.
And what is a caregiver?
A caregiver is an unpaid family or non-family member helping manage the daily life, health, safety, and care of a person living with dementia.
That may be a spouse.
An adult child.
A daughter-in-law.
A sibling.
A friend.
A neighbor.
Someone helping with medications, meals, showers, transportation, finances, appointments, safety, wandering, and behavior changes.
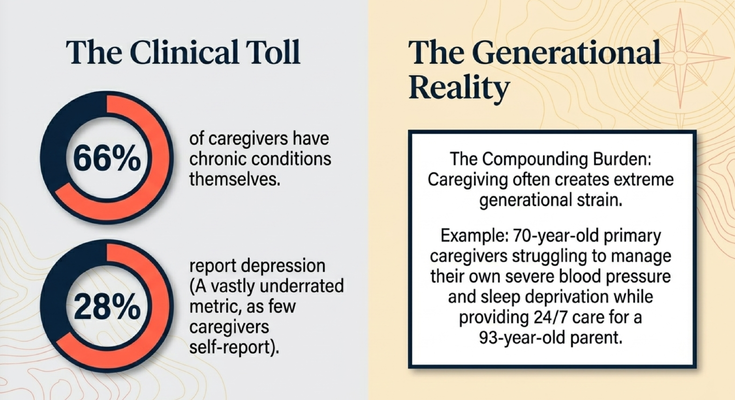
And many caregivers are struggling with their own health.
A large percentage have chronic conditions themselves.
Many report depression.
And I believe that depression number is underreported. Because how many caregivers walk around saying, “Please survey me, I am depressed”?
Most do not.
They say, “I’m fine.”
They say, “I have to do this.”
They say, “Nobody else can do it.”
They keep carrying the weight until their own body starts breaking down.
My parents are caregivers for my grandmother.
My grandmother is 93. My parents are around 70. And they are managing their own health while caring for her.
That is not easy.
A 70-year-old taking care of a 93-year-old is not a small thing.
So when we talk about dementia diagnosis, we cannot only ask, “What stage is the patient in?”
We also have to ask:
“What is happening to the caregiver?”
Because if the caregiver collapses, the care environment collapses.
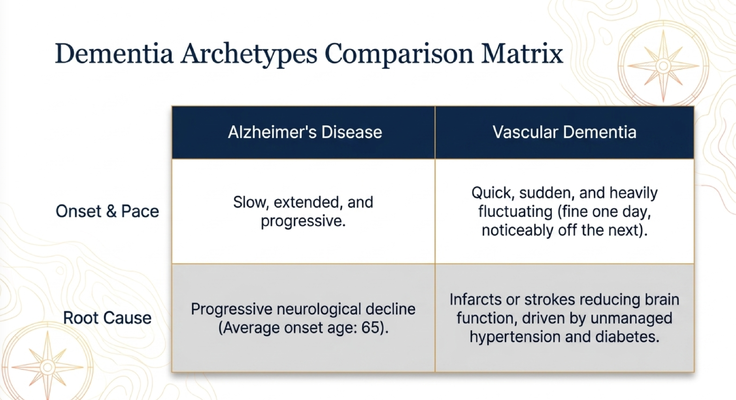
NOT ALL DEMENTIA LOOKS THE SAME
Another reason diagnosis matters is that not all dementia behaves the same way.
Alzheimer’s disease is typically slow and progressive. The changes often happen over years.
But vascular dementia can look different.
Vascular has to do with blood vessels. A person with uncontrolled high blood pressure, diabetes, strokes, or vascular disease may experience changes related to damage in the brain from infarcts or strokes.
So a family may say:
“Mom was okay, and then two days later she was noticeably different.”
That kind of sudden or stepwise change should make us think differently.
Now, not every sudden change is vascular dementia. Sudden confusion can also be delirium from infection, dehydration, medication effects, constipation, pain, or another acute medical problem. So sudden change should always be taken seriously.
But the bigger point is this:
The type of dementia matters.
The stage matters.
The pattern matters.
The timeline matters.
Families need more than the word “dementia.”
They need to understand what kind of dementia is suspected, what stage the person is in, what the pattern looks like, and what decisions need to happen next.
WHY STAGING MATTERS
The doctor may tell you, “Your mom has dementia.”
But that is not enough.
The next question is:
“What stage?”
Early?
Middle?
Late?
Mild?
Moderate?
Severe?
Because caregiver planning changes at every stage.
In early stage, you focus on monitoring, diagnosis confirmation, legal planning, driving conversations, safety planning, and early intervention.
In middle stage, you focus more heavily on safety, behavior, caregiver support, daily assistance, medication reliability, wandering risk, bathing, dressing, and supervision.
In late stage, you focus on full dependency, comfort, advanced care management, swallowing, skin care, infection risk, goals of care, and dignity.
So staging is not about labeling the person.
It is about giving the family a clinical compass.
What should we be worried about now?
What can wait?
What cannot wait?
What decisions need to be made while the person can still participate?
What support does the caregiver need before the next crisis?
If a family does not know the stage, they are often guessing.
And guessing is dangerous in dementia care.
THE PROBLEM WITH QUICK MEMORY SCREENS
Many families have seen some version of a quick memory screen.
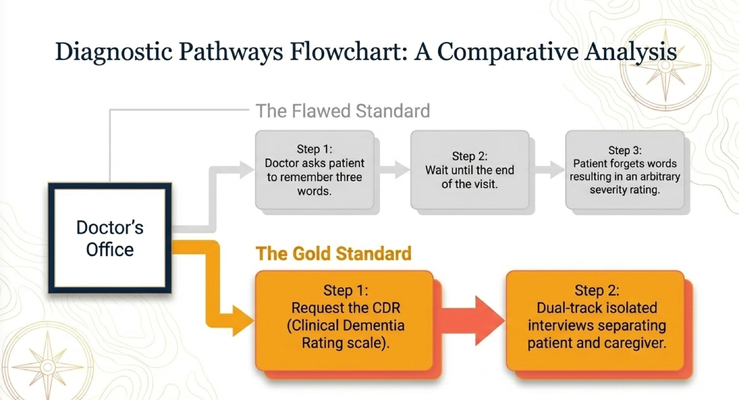
The doctor gives the person three words.
They ask questions.
They wait until the end of the visit.
Then they ask the person to remember the words.
And depending on what the person remembers, they rate the memory.
Now, can that give you some information?
Yes.
But is that the best way to stage dementia?
No.
It is not enough.
Because dementia is not only about remembering three words.
Dementia affects daily function. It affects safety. It affects judgment. It affects finances. It affects medication management. It affects bathing, dressing, toileting, driving, cooking, wandering, sleep, and caregiver burden.
A person may perform okay on a brief test in the office but still be struggling at home.
Or they may perform poorly in the office because they are anxious, tired, hard of hearing, visually impaired, or having a bad day.
So we need better assessment.
One tool families can ask about is the Clinical Dementia Rating scale, or CDR.
THE CLINICAL DEMENTIA RATING SCALE
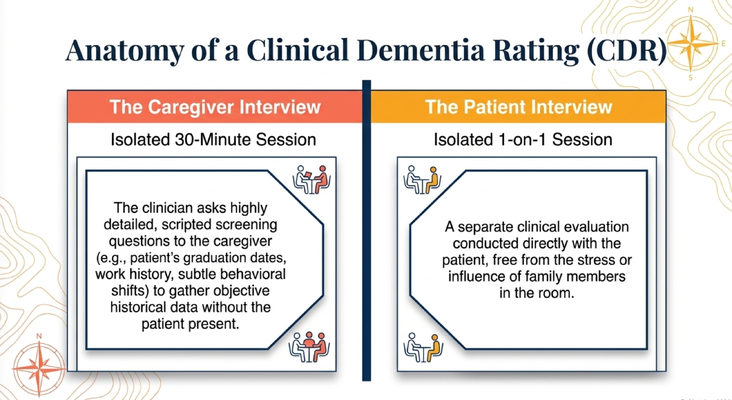
The CDR is valuable because it does not only rely on one quick patient screen.
It involves structured questions and a better understanding of the person’s real-life function.
One part involves speaking with the caregiver.
Why?
Because the caregiver knows the baseline.
The caregiver knows where Mom went to school.
What kind of work she did.
What changed.
What she used to manage independently.
What she can no longer do.
Whether she is missing medications.
Whether she is getting lost.
Whether she is managing money safely.
Whether bathing has changed.
Whether the home is becoming unsafe.
Then the patient is interviewed separately.
That matters too.
Because you do not want family stress, family influence, or embarrassment changing what the patient says. You want to evaluate the person directly while also respecting the caregiver’s historical knowledge.
That dual-track approach gives a more complete picture.
And for caregivers, this is important because you can ask the doctor:
“Can we do a more complete staging assessment?”
“Can we use something like the CDR?”
“Can we talk about whether this is mild, moderate, or severe?”
“Can we connect the stage to what we should be doing next?”
Those are good questions.
Those are advocacy questions.
WHAT CAREGIVERS SHOULD TAKE FROM THIS
If you are a caregiver reading this, here is what I want you to remember.
Do not ignore early signs.
Do not accept “just normal aging” if your gut tells you something has changed.
Ask for an evaluation.
Ask about reversible causes.
Ask what type of dementia is suspected.
Ask what stage your loved one is in.
Ask how the stage changes the care plan.
Ask what decisions need to happen now.
Ask what support exists for the caregiver.
And when the doctor gives you a diagnosis, do not stop there.
Ask:
“What do we do next?”
Because diagnosis without guidance leaves families scared and stuck.
A diagnosis should open the door to planning.
It should lead to education.
It should lead to safety conversations.
It should lead to caregiver support.
It should lead to a plan.
And it should happen early enough that the person living with dementia can still have a voice in the decisions that affect their life.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why caregivers should not have to navigate dementia care alone.
Through the GUIDE Model — Guiding an Improved Dementia Experience — eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because families need more than a diagnosis.
They need help understanding what stage they are in.
They need help preparing for what comes next.
They need help protecting caregiver health.
They need help asking better questions.
They need help connecting the diagnosis to real decisions inside the home.
That is the difference between knowing the word “dementia” and actually having a dementia care plan.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia diagnosis, early screening, staging, caregiver support, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, diagnosis, blood-based screening, treatment eligibility, staging, medications, driving, legal planning, caregiver health, and safety concerns should be discussed with qualified healthcare professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health