
But because this is The Dementia Times, I want to frame the conversation through dementia care.
Because innovation only matters if it reaches the people who need it.
It is not enough to have a great idea.
It is not enough to have a new platform.
It is not enough to have a dashboard, AI tool, early screening method, care model, or workflow.
The real test is this:
Does it get adopted?
Does it reach the family?
Does it help the caregiver?
Does it make the system easier to navigate for the person living with dementia?
Does it work inside the reality of the home?
That is the real test.
DEMENTIA CARE ALREADY LIVES IN FRAGMENTATION
Before we talk about technology, we have to talk about the reality families already live in.
Dementia care is fragmented.
The primary care doctor is over here.
The neurologist is over there.
The psychiatrist may be somewhere else.
The hospital discharge paperwork says one thing.
The home care agency sees something different.
The pharmacy has its own medication list.
The caregiver is standing in the middle trying to hold it all together.
And too often, the caregiver becomes the only glue in the system.
That is not a small problem.
Because dementia does not stay neatly inside a doctor’s office.
It shows up at home.
It shows up in the kitchen.
It shows up in the bathroom.
It shows up at 10 PM when the person living with dementia is seeing shadows.
It shows up after discharge when the family has paperwork they do not understand.
It shows up when Mom refuses a shower or Dad will not take medication.
So when someone says, “We have a new healthcare innovation,” my first question is not only:
“Is the idea good?”
My question is:
“Will this actually make life easier for the person living with dementia and the caregiver?”
Because if we introduce innovation but nobody adopts it, we have not solved a problem.
We have added another burden.

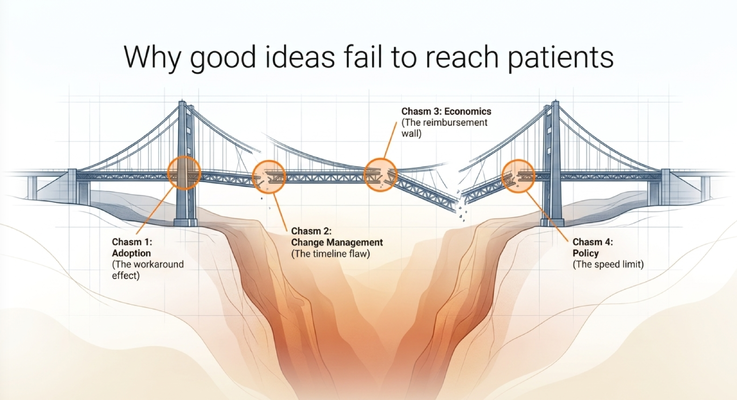
WHY GOOD IDEAS FAIL
One of the clearest themes from the panel was this:
Good ideas do not automatically survive healthcare.
There are barriers they have to cross.
Adoption.
Change management.
Economics.
Policy.
Procurement.
Reimbursement.
Trust.
Clinical relevance.
End-user experience.
That is why healthcare innovation is hard.
A technology may look beautiful in a demo, but once it enters a real organization, the question becomes:
Will the staff use it?
Will it fit the workflow?
Will it integrate with existing systems?
Will it improve outcomes?
Will the economics make sense?
Will policy support it?
Will it survive six months after go-live?
Will it still be used when the excitement wears off?
That is where many good ideas fail.
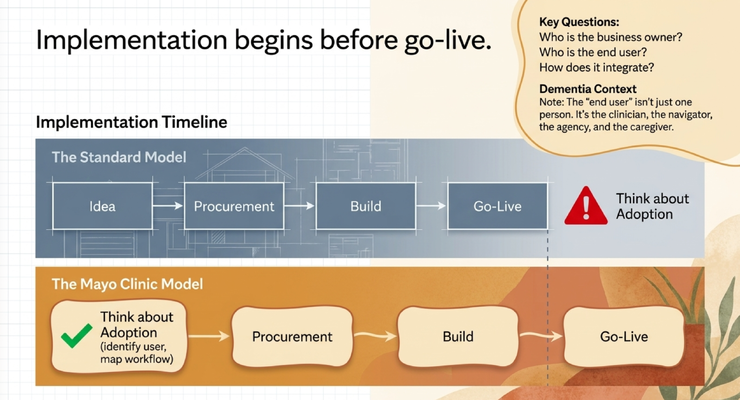
And in dementia care, the stakes are even higher because the end user is not just one person.
Sometimes the end user is the clinician.
Sometimes it is the care navigator.
Sometimes it is the home care agency.
Sometimes it is the caregiver.
Sometimes it is the person living with dementia.
If the innovation does not fit that ecosystem, it will not reach the family.
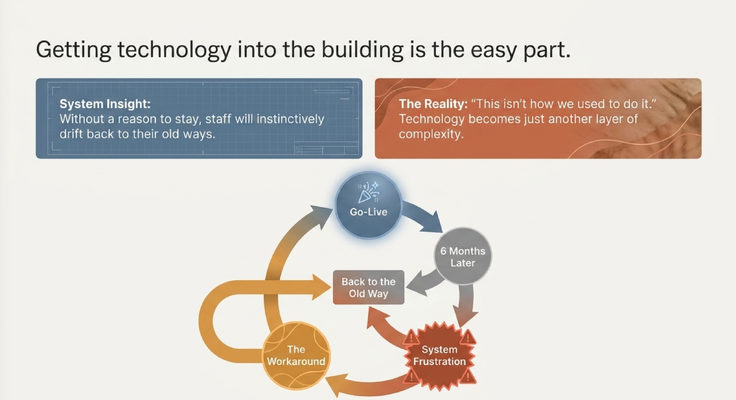
GETTING TECHNOLOGY INTO THE BUILDING IS THE EASY PART
One of the major points from the discussion was that getting technology into the building is often not the hardest part.
The hard part is adoption.
A health system can purchase a platform, launch a new system, train the staff, and celebrate go-live.
Everyone may be excited at first.
The first few months may feel promising.
But then six months later, eight months later, twelve months later, people can start drifting back to the old way.
They create workarounds.
They use the new system halfway and the old system halfway.
They say:
“This is not how we used to do it.”
And now the innovation that was supposed to simplify the workflow becomes another layer of complexity.
That is a problem in any part of healthcare.
But in dementia care, it is especially dangerous.
Because families are already dealing with fragmented systems.
If we add another tool that nobody uses correctly, the caregiver does not feel more supported.
The caregiver feels more confused.
That is why adoption has to be designed, not assumed.
IMPLEMENTATION BEGINS BEFORE GO-LIVE
Another major theme was that implementation has to begin before go-live.
You do not wait until the technology is already installed to start thinking about change management.
You plan early.
Who owns the problem?
Who is the end user?
What workflow is changing?
How does the technology integrate with the existing system?
Is this scalable?
Is this redundant?
Who needs training?
Who needs to buy in?
What happens after launch?
That is the discipline healthcare innovation needs.
And again, in dementia care, this matters because the end user is not simple.
If you are building or implementing a dementia care solution, you have to ask:
Can the caregiver actually use it?
Will the care navigator use it?
Will the physician trust it?
Will the home care agency understand it?
Will it help after hospital discharge?
Will it work when the caregiver is overwhelmed, sleep-deprived, and trying to manage real behaviors in the home?
If the answer is no, then the idea may be technically impressive but practically useless.
Innovation has to be built around real life.
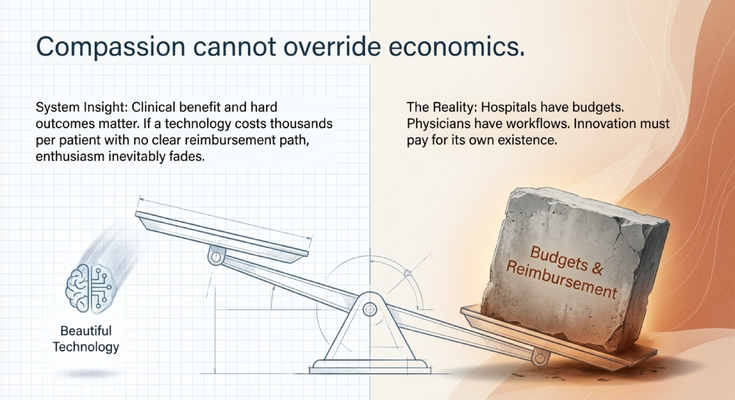
COMPASSION CANNOT OVERRIDE ECONOMICS
Another important point from the panel was very practical:
Clinical benefit matters.
Hard outcomes matter.
Reimbursement matters.
The economics have to make sense.
And I know some people do not like hearing that.
They say, “But this helps patients.”
That matters. Of course it matters.
But hospitals have budgets.
Physicians have workflows.
Health systems cannot absorb unlimited cost forever.
If a technology costs thousands of dollars per patient and there is no reimbursement path, enthusiasm starts to fade.
That is not lack of compassion.
That is healthcare reality.
If the economics do not work, the innovation often does not scale.
And this is one of the biggest lessons for dementia care.
We can have better screening tools.
We can have better care navigation.
We can have better support models.
We can have better technology.
But if reimbursement does not support them, access becomes limited.
And when access is limited, families lose time.
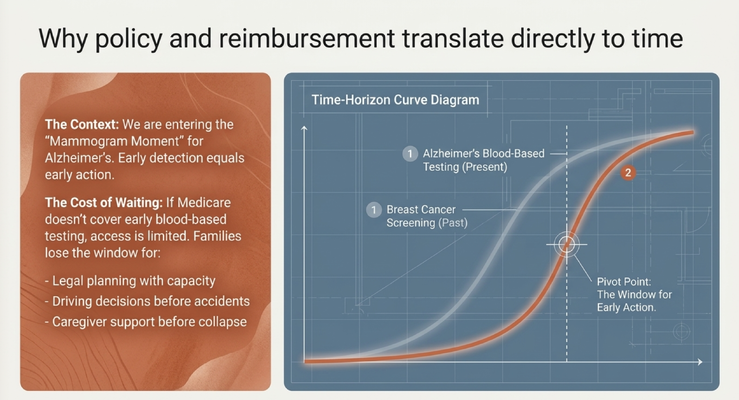
POLICY AND REIMBURSEMENT TRANSLATE DIRECTLY TO TIME
This is where dementia care becomes very real for me.
I recently came back from Washington, D.C., where we were advocating for Alzheimer’s screening and prevention.
I call this our mammogram moment.
Think about breast cancer screening. Earlier screening changed the way families approached the disease. The earlier you know, the earlier you can plan, treat, and act.
Alzheimer’s disease is entering a similar moment.
We now have blood-based testing that may help identify Alzheimer’s-related risk earlier. But if Medicare does not support access, then access becomes limited.
And in dementia care, limited access is not just an administrative issue.
It is time lost.
Time to plan.
Time to talk about driving.
Time to talk about legal documents.
Time to discuss power of attorney.
Time to consider treatment options when appropriate.
Time to support the caregiver before collapse.
Time to have difficult conversations before the family is trapped in difficult situations.
That is why reimbursement matters.
That is why policy matters.
Because policy and reimbursement translate directly to time for families.
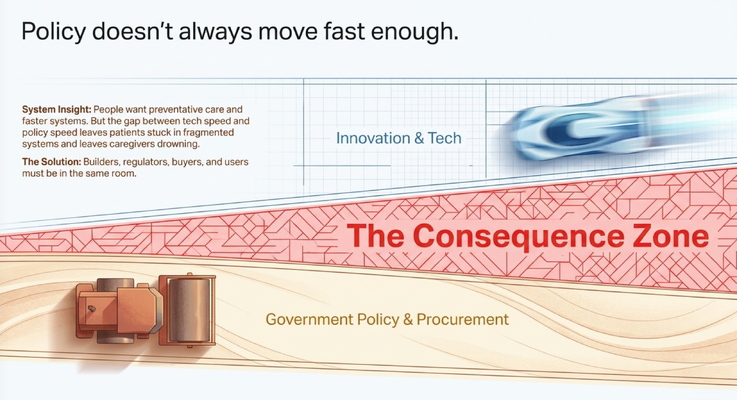
POLICY DOES NOT ALWAYS MOVE FAST ENOUGH
Another theme from the conversation was that policy does not always move as fast as innovation.
People want access to better care.
They want preventative care.
They want faster systems.
They want innovation that reaches them before crisis.
But government, procurement, reimbursement, and policy can move slowly.
That gap has consequences.
If technology moves fast but policy moves slowly, families can stay stuck.
If we have better screening but access is delayed, families wait.
If we have promising tools but procurement takes too long, health systems cannot move.
If builders, regulators, buyers, clinicians, and users are not in the same room, everyone keeps solving only one part of the problem.
That is why events like World Health Expo Miami matter.
Rooms like this matter.
Conversations like this matter.
Healthcare cannot be changed by one group alone.
The builder needs to understand the health system.
The health system needs to understand the caregiver.
The policymaker needs to understand the clinical reality.
The clinician needs to understand the workflow.
The caregiver needs to be heard.
And the person living with dementia has to remain at the center.
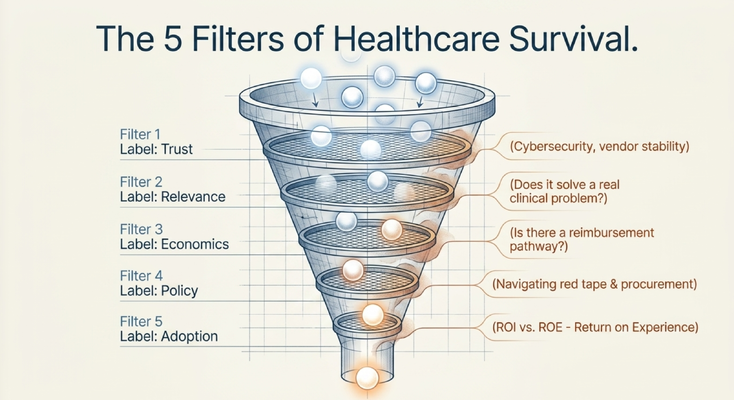
THE FIVE FILTERS HEALTHCARE INNOVATION HAS TO SURVIVE
If I had to summarize the conversation, I would say healthcare innovation has to survive five filters.
Trust.
Relevance.
Economics.
Policy.
Adoption.
Trust means the organization has to believe the solution is safe, stable, secure, and credible.
Relevance means the innovation must solve a real clinical or operational problem.
Economics means the cost, reimbursement, and financial logic have to make sense.
Policy means the solution has to survive regulation, procurement, and system-level rules.
Adoption means the people expected to use it must actually use it.
That last one is critical.
Because an unused innovation is not innovation.
It is decoration.
And dementia care cannot afford decoration.
Families do not need impressive ideas that never touch their lives.
They need support that works.
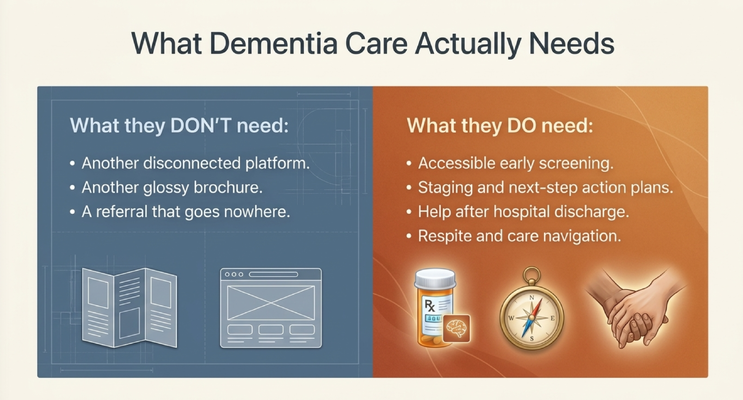
WHAT DEMENTIA CARE ACTUALLY NEEDS
Now let’s bring this back to dementia.
Dementia care does not need another disconnected platform.
It does not need another glossy brochure.
It does not need another referral that goes nowhere.
It does not need innovation that looks impressive in a boardroom but fails in the home.
What dementia care actually needs is practical.
Accessible early screening.
Accurate staging.
Next-step action plans.
Medication review.
Help after hospital discharge.
Respite.
Care navigation.
Support when behaviors happen at home.
Caregiver education.
A system that recognizes the caregiver as part of the care plan.
Because the caregiver is not extra.
The caregiver is the infrastructure.
If Mom refuses a shower, the family needs help.
If Dad is seeing shadows at 10 PM, the family needs help.
If the caregiver is staring at discharge papers they do not understand, they need help.
If the family is trying to manage medications from multiple doctors, they need help.
If the caregiver is exhausted, isolated, depressed, and physically worn down, they need help.
That is where innovation has to land.
Not only inside the hospital.
Inside the home.
THE GUIDE MODEL AND CONNECTED CARE
This is exactly why I believe so strongly in the GUIDE Model.
The GUIDE Model — Guiding an Improved Dementia Experience — is not only a program.
It represents a shift in how Medicare thinks about dementia care.
Instead of treating only the individual patient, it recognizes the patient and caregiver together.
That matters.
Because dementia care is not only about memory loss.
It is about safety.
It is about behavior.
It is about home life.
It is about caregiver health.
It is about medication confusion.
It is about hospital transitions.
It is about what happens when the doctor visit ends and the family goes home.
Through the GUIDE Model, eligible families may receive structured dementia-care support through MedBetter Health.
That support may include:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This is the kind of innovation dementia care needs.
Not disconnected.
Connected.
Not theoretical.
Practical.
Not only built for the clinic.
Built for the family.
BEGIN WITH THE END IN MIND
One of the things I said during the panel is this:
Begin with the end in mind.
If you are a healthcare innovator, do not start only with your technology.
Start with the problem.
Start with the patient.
Start with the caregiver.
Start with the workflow.
Start with the reimbursement reality.
Start with the adoption problem.
Start with the question:
What are we actually solving, and will this still work six months after go-live?
That is the difference between an idea and implementation.
And in dementia care, implementation is everything.
Because the family does not need an impressive concept.
The family needs support that works when the crisis happens.
THE HUMAN SIDE OF ADVOCACY
Toward the end of the panel, I shared a story from Washington.
During an Alzheimer’s advocacy trip, there was a gentleman living with Alzheimer’s disease.
He was around 60 when he was diagnosed.
His son was diagnosed even younger.
He was speaking directly to a senator and saying:
“If I only would have known earlier, I could have planned so many things.”
You could see the senator’s face change.
Because at the end of the day, policymakers are people too.
Healthcare executives are people too.
Innovators are people too.
Sometimes, the data matters.
But sometimes, the story makes the data real.
That is why advocacy matters.
That is why being in the room matters.
That is why caregivers and families have to be part of the conversation.
Healthcare innovation should not be designed only around what the system wants to build.
It should be designed around what families actually need.
A sincere thank you to Steven Travers, Roberto J. Gonzalez, Himakshi Jhala, and Yiannis S. Chatzizisis for sharing your time, expertise, and perspective on this panel.
Conversations like this matter because healthcare innovation cannot improve lives if the people building, buying, regulating, implementing, and using these systems are not in the same room.
WHAT I WANT PROFESSIONALS TO TAKE FROM THIS
If you are a healthcare professional, hospital leader, policymaker, home care agency owner, innovator, investor, researcher, or clinician reading this, here is what I want you to remember:
Healthcare innovation must survive reality.
Not theory.
Reality.
The physician’s workflow.
The caregiver’s exhaustion.
The hospital’s procurement process.
The reimbursement pathway.
The policy timeline.
The end user’s trust.
The patient’s safety.
The family’s ability to actually use the support.
If an innovation does not survive reality, it does not matter how good it looks.
And in dementia care, reality is often happening at home.
It is happening when the caregiver is alone.
It is happening after the hospital discharge.
It is happening when the aide calls and says, “I cannot manage this.”
It is happening when the family does not know whether to call the doctor, go to the ER, or wait.
That is where innovation has to work.
That is where healthcare has to improve.
And that is where dementia care has to go next.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, caregiver support, early detection, care navigation, and practical strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, diagnosis, blood-based screening, treatment options, care planning, medication concerns, caregiver burnout, safety concerns, and eligibility for care programs should be discussed with qualified healthcare professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health