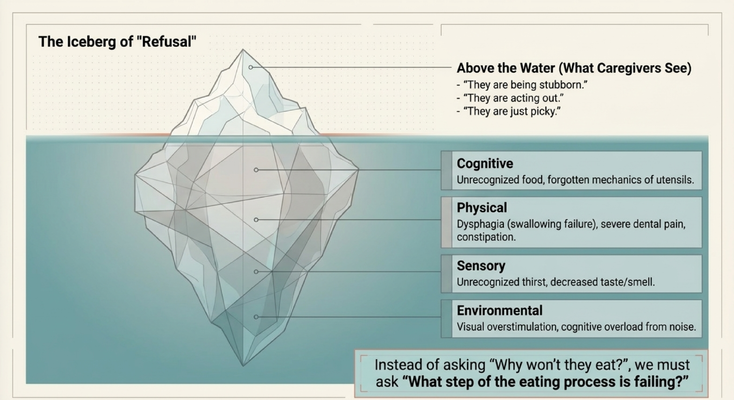
THE ICEBERG OF “REFUSAL”
Let’s start with the iceberg.
Above the water is what the caregiver sees.
Dad is not eating.
Mom is spitting food out.
Your loved one is pushing the plate away.
They are pocketing food in the cheeks.
They are refusing water.
They are coughing during meals.
And above the surface, it is very easy to label the behavior:
“They are being stubborn.”
“They are acting out.”
“They are just picky.”
But below the surface, there may be a much more serious explanation.
There may be a cognitive problem. The person may not recognize the food anymore. They may not understand what the fork is for. They may not know how to begin the sequence of eating.
There may be a physical problem. Dental pain, loose dentures, constipation, nausea, medication side effects, swallowing fatigue, or dysphagia may be making eating uncomfortable or unsafe.
There may be a sensory problem. The person may not feel thirst normally anymore. Food may taste bland. Food may not visually stand out from the plate. Smell may be reduced. Vision may be reduced.
There may be an environmental problem. The room may be too loud. The plate may be visually cluttered. Too many people may be talking. The television may be on. The person may be overwhelmed before the meal even begins.
That is why we cannot stop at the surface.
Behavior is communication.
And at mealtime, refusal may be the body communicating what the brain can no longer explain.
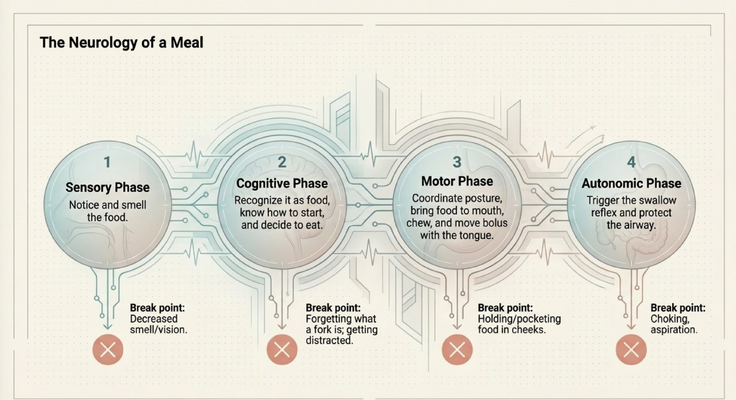
THE NEUROLOGY OF A MEAL
Eating looks simple because we do it automatically.
But when you slow it down, a meal is actually a highly coordinated neurological event.
First, there is the sensory phase.
You have to notice the food. You have to see it. You have to smell it. You have to recognize that something edible is in front of you.
That alone can break down in dementia.
If vision changes, smell decreases, or food blends into the plate, the person may not even register the meal the way you and I do.
Second, there is the cognitive phase.
The person has to recognize that the object in front of them is food. They have to understand what the fork is. They have to know what to do next. They have to decide to begin.
In dementia, that sequence can break down.
So the food is there, but the brain does not know how to start.
Third, there is the motor phase.
The person has to sit upright, coordinate posture, pick up the fork, bring food to the mouth, chew, move the food with the tongue, and prepare it to swallow.
That requires planning, strength, coordination, attention, and timing.
When that breaks down, you may see food pocketing. They hold food in the cheeks. They chew slowly. They forget what to do with the food once it is in the mouth.
Fourth, there is the autonomic phase.
This is where swallowing has to happen safely. The swallow reflex has to trigger, and the airway has to be protected so food goes down the esophagus, not into the lungs.
That is not a small detail.
That is safety.
Because when food, liquid, or saliva enters the airway, we start thinking about aspiration.
And aspiration can lead to pneumonia.
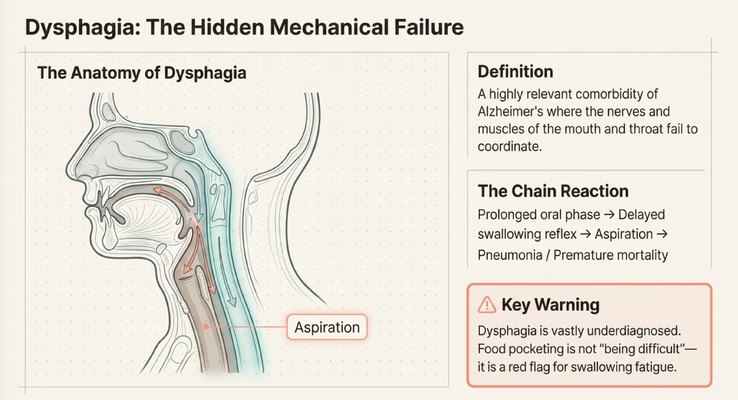
WHEN SWALLOWING BECOMES THE PROBLEM
Now let’s talk about dysphagia.
Dysphagia means difficulty swallowing.
In dementia and Alzheimer’s disease, dysphagia can happen when the nerves and muscles of the mouth and throat no longer coordinate properly. The person may want to eat. They may be hungry. They may even accept the food into the mouth.
But the swallow sequence is not working the way it should.
So what does the caregiver see?
Food sitting in the cheek.
Long chewing without swallowing.
Coughing during meals.
A wet or gurgly voice after eating or drinking.
Fear around swallowing.
Recurrent pneumonia.
Weight loss.
Dehydration.
And sometimes the caregiver says:
“They just won’t swallow.”
But the person may not be trying to be difficult.
They may be afraid.
Imagine every time you swallow, you cough or choke. Imagine your body has learned that swallowing feels dangerous. Now someone keeps saying, “Swallow. Come on. Swallow.”
That does not feel comforting.
That feels frightening.
Food pocketing is not always stubbornness.
It can be a red flag for swallowing fatigue or dysphagia.
And if your loved one coughs repeatedly during meals, develops a wet or gurgly voice after swallowing, has recurrent chest infections, or seems to be aspirating, that needs medical attention. Speak with the physician. Ask whether a swallowing evaluation is needed. Ask whether a speech-language pathologist should be involved.
Do not force fluids or food if swallowing seems unsafe.
Slow down and get guidance.
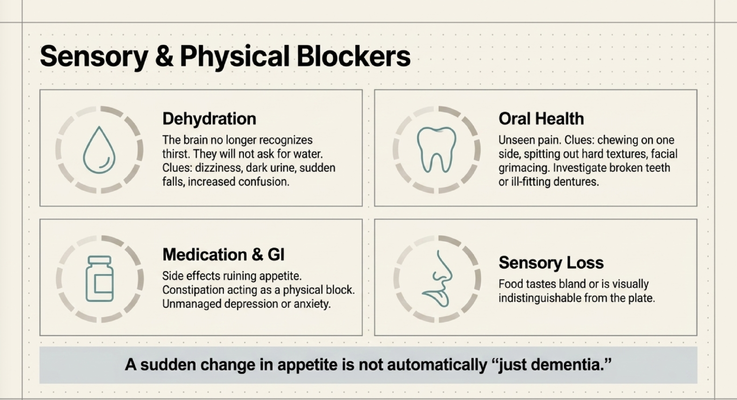
THE HIDDEN BLOCKERS: THIRST, TEETH, MEDICATIONS, AND SENSORY LOSS
There are also several blockers caregivers may not immediately see.
The first is dehydration.
In a healthy brain, thirst creates a signal: “I need water.”
But in dementia, that signal may weaken or disappear. Your loved one may not ask for water. They may not recognize thirst. They may become dizzy, more confused, weak, or more prone to falls. Urine may become darker. The caregiver may think the dementia is suddenly worse, when dehydration may be contributing.
The second is oral health.
A person living with dementia may not be able to say, “My tooth hurts.” They may not be able to explain that dentures are loose, a tooth is broken, or chewing on one side causes pain.
So instead of saying, “My mouth hurts,” they spit out hard textures. They chew only on one side. They grimace. They refuse certain foods.
That is not picky eating.
That may be pain.
The third is medication and gastrointestinal issues.
Certain medications can affect appetite, taste, nausea, alertness, constipation, or dry mouth. Constipation itself can reduce appetite and make the person uncomfortable. Depression and anxiety can also affect eating.
So if appetite suddenly changes, ask the doctor to review the medication list and the full medical picture.
The fourth is sensory loss.
Food may taste bland. Smell may be reduced. The food may visually blend into the plate. If mashed potatoes are on a white plate, the person may not clearly see the food. If the table is cluttered and noisy, they may not know where to focus.
That is why a sudden change in appetite should not be dismissed as “just dementia.”
It may be dementia.
But it may also be dehydration, dental pain, constipation, medication side effects, sensory loss, swallowing difficulty, infection, depression, or another medical issue that needs attention.
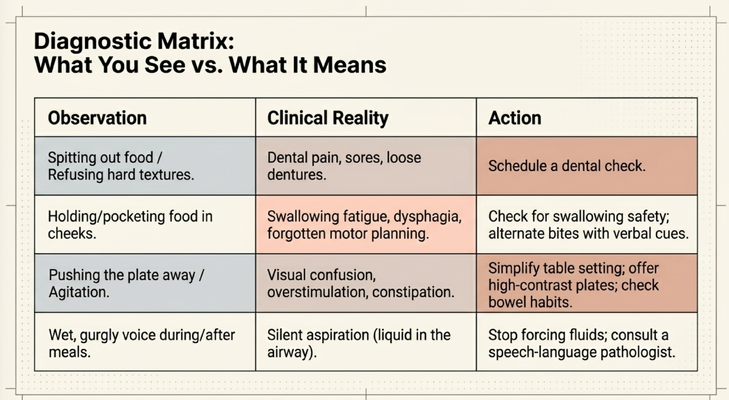
WHAT YOU SEE VERSUS WHAT IT MAY MEAN
Caregivers need a practical way to interpret what they are seeing.
If your loved one is spitting out food or refusing hard textures, think about dental pain, mouth sores, loose dentures, or difficulty chewing. The next step may be a dental check.
If they are holding food or pocketing it in the cheeks, think about swallowing fatigue, dysphagia, or forgotten motor planning. The next step may be a swallowing-safety evaluation and a conversation with the medical team.
If they are pushing the plate away or becoming agitated, think about visual confusion, overstimulation, constipation, pain, or the environment. The next step may be simplifying the table, reducing noise, improving contrast, checking bowel habits, and making the meal less overwhelming.
If they have a wet or gurgly voice during or after meals, think about possible aspiration. Liquid may be entering the airway. The next step is not to push harder. The next step is to stop, slow down, and speak with a clinician. A speech-language pathologist may need to evaluate swallowing safety.
That is the shift I want families to make.
Do not only ask, “How do I get them to eat?”
Ask:
“What am I seeing?”
“What could it mean?”
“What is the safest next step?”
That is how mealtime becomes clinical observation instead of a battle.
MEDICAL RED FLAGS CAREGIVERS SHOULD NOT IGNORE
There are certain signs that should not be brushed off.
Coughing or choking during meals.
A wet or gurgly voice after swallowing.
Recurrent chest infections or pneumonia.
Unexplained fever, especially after choking episodes.
Rapid, unexplained weight loss.
Signs of severe dehydration.
Sudden worsening of confusion.
Sudden refusal of all fluids.
These are not moments to say, “Well, it is probably just dementia.”
Sudden eating and drinking changes can be medical.
They can involve swallowing safety.
They can involve infection.
They can involve dehydration.
They can involve medication side effects.
They can involve pain.
They can involve a level of risk that needs review.
So yes, we want to be calm. We want to be practical. We do not want to panic every time something changes.
But we also do not ignore the red flags.
If symptoms are sudden, severe, dangerous, or associated with choking, coughing, dehydration, fever, recurrent pneumonia, or rapid decline, contact the appropriate medical professionals promptly.
THE GOAL IS NOT TO WIN THE MEALTIME BATTLE
I want caregivers to hear this clearly:
The goal is not to win a mealtime battle.
The goal is to understand what is making eating hard.
If the person does not recognize the food, we adapt.
If the room is too loud, we simplify.
If the plate does not provide enough contrast, we change the plate.
If utensils are confusing, we consider familiar finger foods when safe.
If hard textures cause pain, we investigate the mouth.
If swallowing looks unsafe, we stop forcing and get clinical guidance.
If the person is overwhelmed, we slow the pace.
If they are pocketing food, we pay attention.
If they cough after drinking, we do not ignore it.
This is the lens of empathy.
Empathy does not mean pretending everything is fine.
It means looking at the behavior and asking:
“What is the unmet need?”
Is it safety?
Comfort?
Nutrition?
Dignity?
Pain?
A swallowing problem?
A sensory problem?
A cognitive problem?
A noisy environment?
Because refusal is often an unmet need.
Whether it is unrecognized food, a hidden toothache, a failing swallow reflex, dehydration, constipation, medication side effects, or a meal environment that is overwhelming, the body is communicating what the brain can no longer explain.
That is dementia care.
Not forcing.
Not arguing.
Not shaming.
Understanding.
Adapting.
Protecting dignity.
And knowing when to bring in the clinical team.
WHAT I WANT CAREGIVERS TO REMEMBER
If you are caring for someone living with dementia, I want you to remember this:
Eating is not one simple action.
It is a chain.
The person has to see the food, smell the food, recognize the food, understand how to start, coordinate posture, use the hands, chew, move food with the tongue, trigger the swallow, and protect the airway.
If any part of that chain breaks, the caregiver may see “refusal.”
But the real problem may be much deeper.
So do not blame yourself if mealtimes have become difficult. And do not immediately blame your loved one either.
Slow down.
Observe.
Look for patterns.
Look for pain.
Look for coughing.
Look for pocketing.
Look for weight loss.
Look for dehydration.
Look at the teeth.
Look at the dentures.
Look at the medication list.
Look at the room.
Look at the plate.
Look at the noise.
Look at whether the person seems afraid.
Then bring those observations to the medical team.
A caregiver who can say, “She pockets food in her left cheek,” or “He coughs every time he drinks water,” or “She spits out hard textures but eats soft foods,” is giving the clinician useful information.
That information matters.
Because the goal is not just to get through one meal.
The goal is safety, dignity, nutrition, comfort, and a care plan that matches what is actually happening.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why dementia families should not have to navigate this alone.
A caregiver may hear all of this and think:
“Dr. Erik, this is helpful, but who is supposed to walk me through this in real life?”
That is the right question.
Most doctors are doing their best, but dementia behaviors and mealtime problems take time. Caregivers need education. They need someone who can help them think through patterns. They need support when eating changes suddenly. They need help knowing what to ask the doctor, when to call the clinician, when swallowing safety may be an issue, and how to make the home environment safer.
That is why the GUIDE Model matters.
GUIDE stands for Guiding an Improved Dementia Experience.
Through the GUIDE Model, eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Medicare-covered respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
For a caregiver dealing with mealtime problems, that support matters.
Because eating changes can be frightening.
Coughing can be frightening.
Weight loss can be frightening.
Pocketing food can be confusing.
And when the caregiver is already exhausted, trying to figure all of this out alone can feel impossible.
Families need more than a diagnosis.
They need guidance.
They need a care plan.
They need support around the person living with dementia and the caregiver holding everything together.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, mealtime challenges, caregiver support, the GUIDE Model, and practical care strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, appetite changes, dehydration, dental pain, dysphagia, aspiration risk, coughing during meals, recurrent pneumonia, medication side effects, weight loss, swallowing safety, caregiver burnout, and nutrition concerns should be discussed with qualified healthcare professionals. If symptoms are sudden, severe, dangerous, or medically concerning, seek immediate medical help.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health