BEHAVIOR IS COMMUNICATION
I want you to remember one sentence:
Behavior is communication.
If your loved one living with dementia is pacing, restless, refusing care, asking repeated questions, or becoming suspicious, they are communicating something.
They may not be able to say, “I am overwhelmed.”
They may not be able to say, “The room looks strange.”
They may not be able to say, “I am hungry.”
They may not be able to say, “My hearing aid battery died and now I am exhausted from trying to understand everyone.”
They may not be able to say, “My back hurts.”
So the message comes out as behavior.
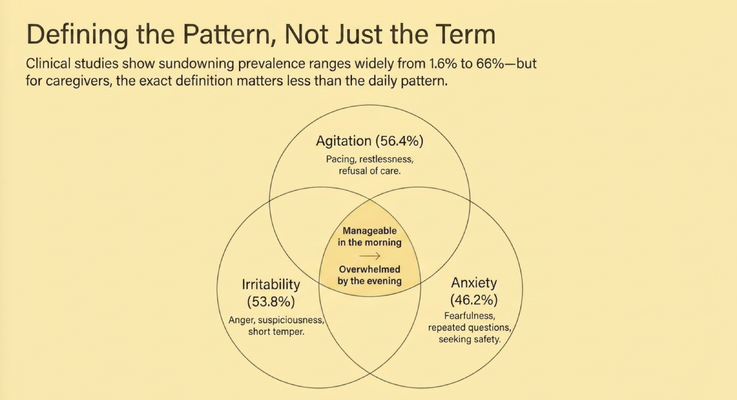
Agitation may look like pacing, restlessness, or refusal of care. Irritability may look like anger, suspicion, or a short temper. Anxiety may look like fearfulness, repeated questions, or constantly seeking safety.
That is why the exact textbook definition of sundowning matters less to the caregiver than the daily pattern.
If every afternoon begins to look the same, pay attention.
The pattern is giving you information.
THE BUILD-UP, NOT THE SWITCH
Many caregivers experience sundowning as if something suddenly changed.
At 2 PM, Mom seemed okay.
At 5 PM, she is pacing, yelling, afraid, or refusing care.
So the caregiver thinks, “It came out of nowhere.”
But most of the time, it did not come out of nowhere.
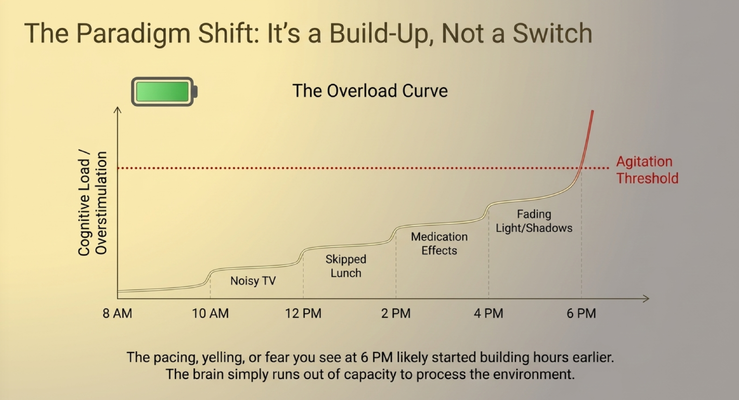
Think of the brain like a battery.
In the morning, the battery may be fuller. The person may tolerate more noise, more movement, more instructions, more decisions, and more activity.
But throughout the day, that battery drains.
The TV is loud.
The room is busy.
Lunch gets skipped or delayed.
There is pain or fatigue.
Medication side effects begin showing up.
The sun starts going down.
Shadows appear.
Reflections in windows look unfamiliar.
The caregiver gets tired and starts rushing.
Each one of those things may seem small by itself. But together, they raise the cognitive load.
And eventually the person crosses the agitation threshold.
That is why the pacing, yelling, fear, or refusal you see at 6 PM may have started building at noon.
The dementia brain simply runs out of capacity to process the environment.
THE 4 PM RESET
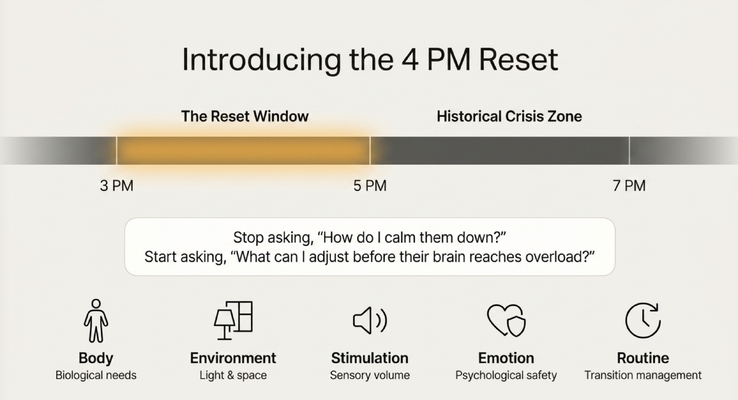
This is where the 4 PM Reset comes in.
The reset is not a magic trick.
It is a prevention window.
Instead of waiting until the crisis zone, we intervene earlier. Around 3 PM to 5 PM, we begin reducing the load before the person reaches overload.
That means we look at five areas:
The body.
The environment.
Stimulation.
Emotional safety.
Routine.
Those five areas become the reset.
Because if the behavior is communication, the caregiver’s job is not just to stop the behavior. The caregiver’s job is to ask what the behavior is trying to say.
What can I adjust before their brain reaches overload?
That is the shift.
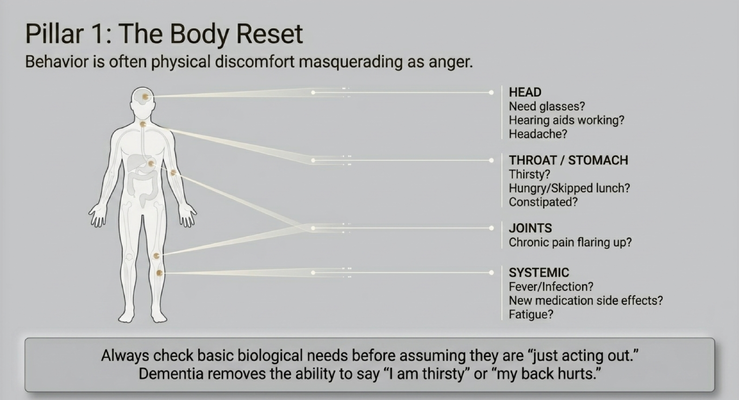
PILLAR 1: THE BODY RESET
The first reset is the body.
Before we assume someone is “just acting out,” we have to check the basics.
Is there pain?
Are they thirsty?
Are they hungry?
Did they skip lunch?
Are they constipated?
Do they have a headache?
Are their glasses on?
Are their hearing aids working?
Are they fatigued?
Could there be a fever, infection, medication side effect, or something new medically?
This matters because behavior is often physical discomfort wearing the mask of anger.
Dementia can take away a person’s ability to clearly say, “I am thirsty,” “I am constipated,” “My back hurts,” or “I cannot hear you.”
So the caregiver sees refusal.
But the body may be saying discomfort.
The caregiver sees anger.
But the body may be saying pain.
The caregiver sees restlessness.
But the body may be saying hunger, thirst, fatigue, or the need to use the bathroom.
So start with the body.
Not because every behavior is medical.
But because you do not want to miss the simple thing.
A snack, water, pain assessment, bathroom check, hearing aid battery, glasses, or medication review may change the entire evening.
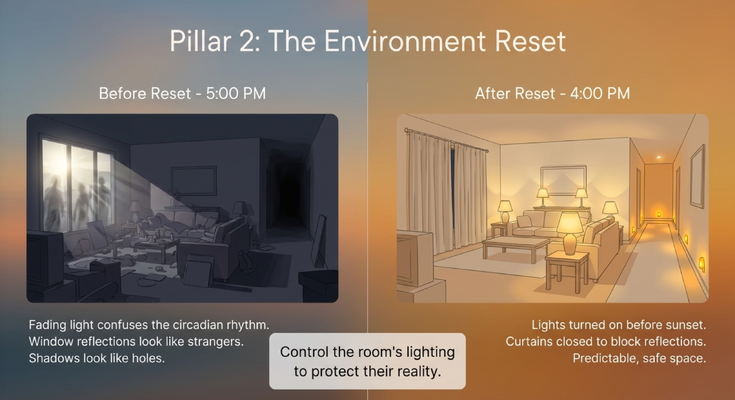
PILLAR 2: THE ENVIRONMENT RESET
The second reset is the environment.
This is one of the biggest ones for sundowning.
As the sun goes down, the room changes.
Light fades.
Shadows stretch.
Windows become reflective.
A coat rack can look like a person.
A dark hallway can look like a hole.
A reflection in the glass can look like a stranger.
To you, the room looks normal.
To a person living with dementia, the same room may suddenly feel unsafe.
That is why you cannot wait until the room is already dark.
Turn on lights before sunset.
Close curtains and blinds before reflections appear.
Reduce clutter.
Create a predictable, calm space.
Use warm lighting.
Use motion-activated lights for hallways, bedrooms, and the path to the bathroom.
That last one is practical. If your loved one gets out of bed at night and the path to the bathroom lights up automatically, you reduce shadows and improve safety at the same time.
Small changes in lighting can make a major difference.
The goal is not to decorate the room.
The goal is to protect their reality.
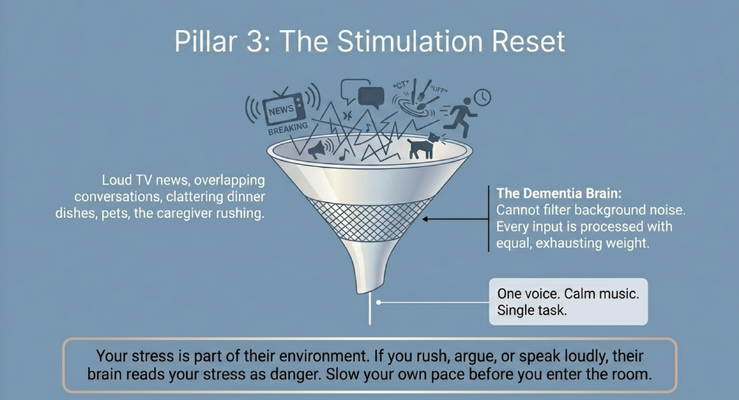
PILLAR 3: THE STIMULATION RESET
The third reset is stimulation.
A dementia brain often cannot filter background noise the way a healthy brain can.
That means everything comes in at once.
The TV.
Breaking news.
Dishes clattering.
People talking over each other.
The dog barking.
Text alerts.
A caregiver rushing.
Dinner being prepared.
The phone ringing.
Music playing.
To you, this may just feel like a normal busy house.
To the person living with dementia, it may feel like every sound has the same weight.
That is exhausting.
And by late afternoon, exhaustion becomes behavior.
So the stimulation reset is simple:
One voice.
Calm music.
One task.
Less noise.
Less movement.
Less rushing.
And here is a part caregivers often miss: your stress is part of their environment.
If you rush into the room, speak loudly, argue, or bring anxiety into your body language, the person living with dementia may mirror that stress.
I see this in my own family.
My parents care for my grandmother, who is 93 going on 94. They love her deeply, but caregiving is stressful. If they walk into the room tense, rushed, or frustrated, my grandmother can feel that energy.
It is like a mirror.
If you smile at the mirror, it smiles back.
If you frown at the mirror, it frowns back.
So before you enter the room, take a breath.
Slow your own pace.
Relax your face.
Lower your voice.
Then walk in.
The reset starts with you.
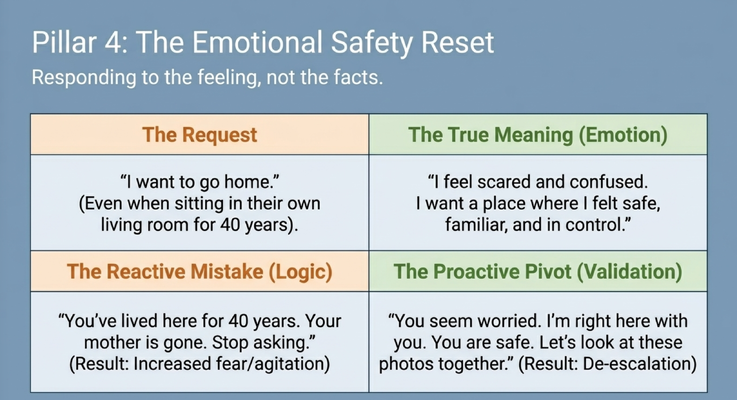
PILLAR 4: THE EMOTIONAL SAFETY RESET
The fourth reset is emotional safety.
This is where a lot of caregivers make the mistake of using facts when the person needs reassurance.
Let’s say Mom is sitting in the living room she has lived in for 40 years.
She says:
“I want to go home.”
The logical response is:
“Mom, you are home. You’ve lived here for 40 years. Your mother is gone. Stop asking.”
But what happens when you say that?
Fear increases.
Agitation increases.
Confusion increases.
Now Mom may feel attacked, corrected, embarrassed, or even more unsafe.
Because “I want to go home” is not always a request for a different address.
Sometimes it means:
“I feel scared.”
“I feel confused.”
“I want a place where I feel safe.”
“I want something familiar.”
“I want control.”
So we respond to the feeling, not only the facts.
“Mom, you seem worried. I’m right here with you. You are safe.”
Then redirect.
“Let’s look at these photos together.”
“Let’s listen to this song.”
“Let’s sit here for a few minutes.”
That is validation.
That is redirection.
That is emotional safety.
You are not trying to win an argument.
You are trying to lower distress.
And in dementia care, lowering distress often matters more than proving the facts.
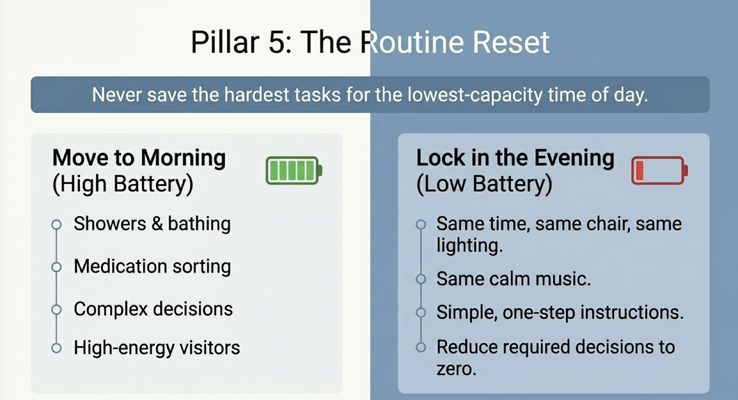
PILLAR 5: THE ROUTINE RESET
The fifth reset is routine.
Never save the hardest tasks for the lowest-capacity time of day.
That one sentence can change the evening.
If showers are difficult, do not force them at 7 PM when the person is already tired, overstimulated, hungry, confused, or anxious.
Move showers and bathing to the morning when the battery is higher.
Move medication sorting to the morning.
Move complex decisions to the morning.
Move high-energy visitors to earlier in the day.
By the evening, the goal should not be productivity.
The goal should be predictability.
Same chair.
Same lighting.
Same calm music.
Same rhythm.
Simple one-step instructions.
Fewer choices.
Less decision-making.
In the evening, do not ask five questions when one calm direction will do. Do not create a debate when the brain is already tired. Do not turn bedtime into a negotiation.
Lock in the evening.
Make it boring in the best possible way.
Because in dementia care, boring can be safe.
Predictable can be calming.
Routine can be medicine for the nervous system.
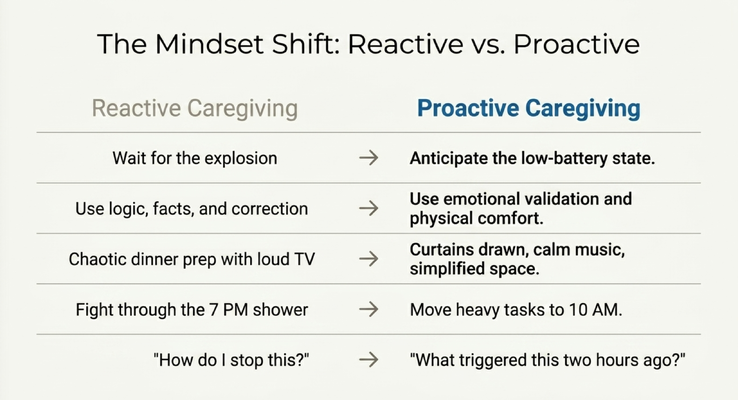
THE MINDSET SHIFT
The real shift is from reactive caregiving to proactive caregiving.
Reactive caregiving waits for the explosion.
Proactive caregiving anticipates the low-battery state.
Reactive caregiving uses logic, facts, and correction.
Proactive caregiving uses emotional validation and physical comfort.
Reactive caregiving keeps the TV loud while dinner is chaotic and everyone is rushing.
Proactive caregiving draws the curtains, lowers the noise, simplifies the space, and slows the pace.
Reactive caregiving fights through the 7 PM shower.
Proactive caregiving moves that shower to 10 AM.
Reactive caregiving asks:
“How do I stop this?”
Proactive caregiving asks:
“What triggered this one or two hours ago?”
That last question is powerful.
I remember a caregiver telling me that his wife was getting frightened at night every Tuesday and Thursday. He could not figure out why it kept happening on those days.
So I asked him:
“What happens on Tuesdays and Thursdays?”
He realized that those were the nights they watched a loud war movie together. Explosions, fighting, noise, chaos. Then later that night, she became scared and felt like she was in danger.
The behavior was not random.
There was an antecedent.
Something came before it.
And once we saw the pattern, we could change the routine.
That is dementia care.
Not just reacting.
Investigating.
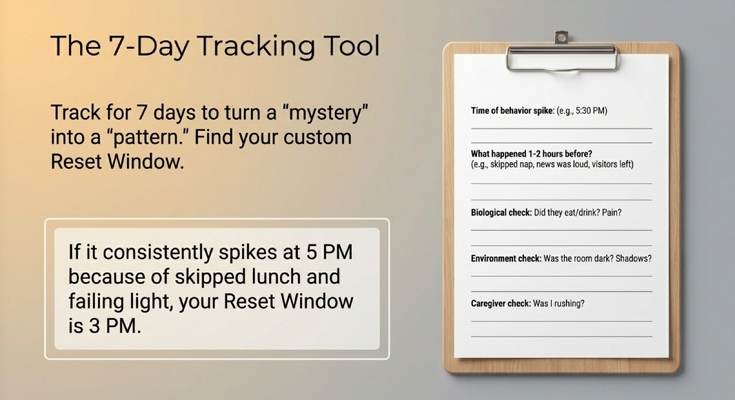
THE 7-DAY TRACKING TOOL
If your loved one spirals every evening, do not only study the moment they explode.
Study the two hours before.
That is where you may find the trigger.
For seven days, track the pattern.
What time did the behavior spike?
What happened one to two hours before?
Did they eat?
Did they drink?
Were they in pain?
Were they constipated?
Was there a bathroom change?
Was the urine different?
Was the room dark?
Were there shadows?
Was there a coat rack, reflection, or hallway that looked frightening?
Was the TV loud?
Were visitors there?
Was the caregiver rushing?
Was I tense when I entered the room?
This is how you turn a mystery into a pattern.
And once you find the pattern, you can find the reset window.
If the behavior spikes at 5 PM because lunch was skipped, the room got dark, and the caregiver rushed in at 4:30, your reset window may be 3 PM.
Not 5 PM.
Not after the explosion.
Before.
That is the golden rule:
If your loved one spirals every evening, do not only study the moment they explode. Study the two hours before. That is where you may find the trigger. And that is where you may be able to change the night.
WHAT CAREGIVERS SHOULD REMEMBER
If you are a caregiver, here is what I want you to take from this.
Sundowning is not usually random. It is often a pattern.
And when you understand the pattern, you can stop waiting for the crisis and start changing the conditions that lead to it.
Check the body first. Hunger, thirst, pain, constipation, hearing, vision, fatigue, medication effects, and infection concerns can all show up as behavior.
Control the environment before the room becomes confusing. Turn on lights before sunset. Close curtains. Reduce shadows. Use motion-activated lights. Make the space predictable.
Reduce stimulation. One voice. Calm music. Less noise. Fewer tasks. Slower pace.
Respond to emotion before facts. If they say, “I want to go home,” hear the fear underneath the words. Validate first. Redirect second.
Move hard tasks to the morning. Do not save showers, medication sorting, complex decisions, or high-energy visitors for the lowest-capacity part of the day.
And track the pattern for seven days.
Not to become perfect.
To become prepared.
Because caregivers do not need more guilt. You already carry enough.
You need a framework.
You need a way to look at the behavior and say:
“What is this communicating?”
“What happened before?”
“What can I adjust earlier?”
That is the 4 PM Reset.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why dementia families should not have to navigate this alone.
A caregiver may watch this and say:
“Dr. Erik, this is helpful, but my doctor’s visit is not set up for this level of detail.”
And that is true.
Most primary care doctors are doing their best. They are managing high blood pressure, diabetes, atrial fibrillation, cholesterol, hospital follow-ups, medications, referrals, and a waiting room full of complex patients.
Dementia behaviors take time.
Caregiver support takes time.
Pattern tracking takes time.
That is one reason the GUIDE Model matters.
GUIDE stands for Guiding an Improved Dementia Experience.
Through the GUIDE Model, eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Medicare-covered respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
Think about what that means for a caregiver dealing with sundowning.
You may have someone to help you walk through the pattern.
Someone to help you think about the body reset, the environment reset, the stimulation reset, the emotional safety reset, and the routine reset.
Someone to call when it is 10 PM and you are not sure what to do.
Someone to help you get respite when you are exhausted.
That is what families need.
Not just a diagnosis.
Not just a pamphlet.
A support system around the person living with dementia and the caregiver holding everything together.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetterHealth currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about sundowning, dementia behaviors, caregiver support, the GUIDE Model, and practical care strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, sudden confusion, agitation, hallucinations, pain, constipation, dehydration, infection symptoms, medication side effects, sleep disruption, caregiver burnout, and safety concerns should be discussed with qualified healthcare professionals. If symptoms are sudden, severe, dangerous, or medically concerning, seek immediate medical help.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health