THE FIGHT HAPPENING IN THOUSANDS OF HOMES
Let’s start with a simple example.
You organize your mother’s medications.
She has ten pills she is supposed to take that day.
You leave in the morning, come back later, and the pills are still there.
So you say:
“Mom, you did not take your medications.”
And she says:
“Yes, I did.”
You show her the pill organizer.
You point to the day of the week.
You count the pills.
You say:
“Mom, look. It says Monday. They are still here.”
And she says:
“No, those are from yesterday. I took mine.”
Now you feel like you are losing your mind.
Because the evidence is right there.
The pills are still in the box.
But in her reality, she took them.
The same thing happens with bills. You see unpaid bills on the table. She says she paid them.
It happens with food. You see spoiled food in the refrigerator. She says everything is fine.
It happens with driving. You see new dents in the car. Dad got lost on the way to a familiar store. He says there is nothing wrong with his driving.
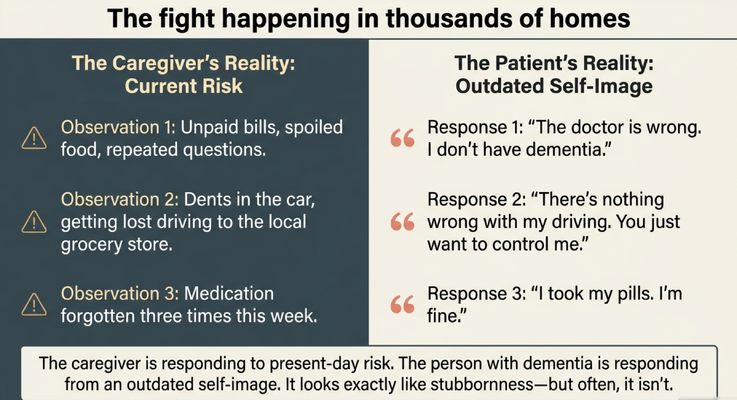
This is the split.
The caregiver sees current risk.
The person living with dementia sees themselves through an older version of who they used to be.
They remember the person who paid every bill on time.
They remember the person who drove everywhere safely.
They remember the person who never missed medication.
They remember the person who was independent.
But the brain may no longer be accurately updating that self-image.
So the caregiver is saying, “Look at what is happening now.”
And the person living with dementia is saying, “I know who I am.”
That is why these conversations become so explosive.
ANOSOGNOSIA: THE WORD CAREGIVERS NEED TO KNOW
The word is anosognosia.
It comes from Greek roots meaning “without knowledge of disease.”
In plain language, anosognosia is a neurological blind spot. It prevents a person from recognizing their own cognitive impairment, memory problems, or functional decline.
This is not the same thing as someone being difficult.
This is not the same thing as someone intentionally lying.
This is not the same thing as a person trying to manipulate you.
Their brain may genuinely not have access to the awareness you are asking them to use.
One way I explain it is with a car dashboard.
Imagine your car is overheating. Everyone outside the car can see steam coming from the engine. They are yelling, “Pull over. Something is wrong.”
But you look at your dashboard, and the gauge says everything is normal.
No warning light.
No overheating.
No problem.
So from your perspective, everyone else is overreacting.
That is what anosognosia can feel like.
Everyone else sees the danger.
But the person’s internal dashboard says, “System normal. No errors detected.”
Before you call it stubbornness, ask whether the brain still has access to the awareness you are asking the person to use.
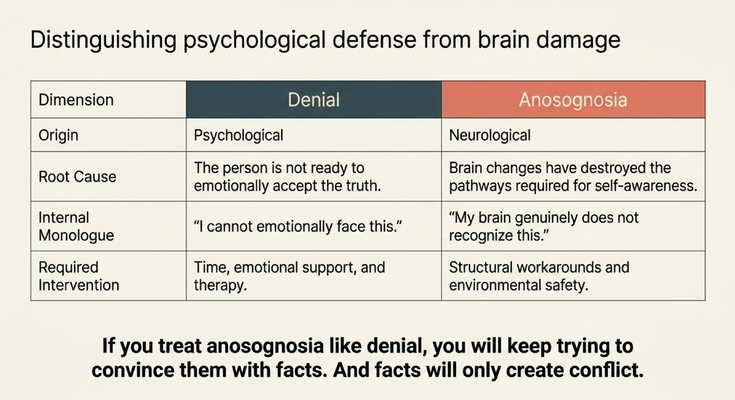
DENIAL IS NOT THE SAME AS ANOSOGNOSIA
This distinction matters.
Denial is psychological.
Anosognosia is neurological.
In denial, the person may understand the truth but is not emotionally ready to face it. The information gets in, but the person pushes it away because it is too painful.
That requires time, emotional support, and sometimes therapy.
But anosognosia is different.
With anosognosia, the brain changes have damaged the networks needed for self-awareness. The person is not simply refusing to accept the truth. The brain may not be able to process the deficit correctly.
That means facts do not land the way you expect them to land.
You can explain.
You can show proof.
You can bring out the pillbox.
You can bring the unpaid bills.
You can show the dents in the car.
You can repeat the diagnosis.
But if the brain cannot recognize the deficit, your evidence may not create insight.
It may create conflict.
That is why treating anosognosia like denial is so dangerous.
If you treat anosognosia like denial, you will keep trying to convince the person with facts.
And facts will only create more fighting.
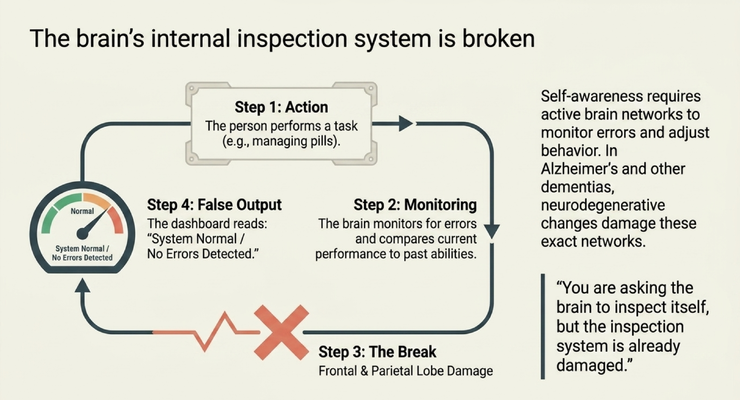
THE BRAIN’S INSPECTION SYSTEM IS BROKEN
Self-awareness requires the brain to monitor itself.
You perform a task.
The brain checks how you did.
It compares your current performance to what you were trying to do.
If there is an error, the brain adjusts.
That is the internal inspection system.
But in Alzheimer’s disease and other dementias, the brain networks involved in awareness, monitoring, and error detection can become damaged.
So the person performs the task incorrectly.
The caregiver sees the error.
But the brain does not register it.
The output still reads:
“Everything is fine.”
That is why medication arguments become so repetitive.
The person may truly believe they took the medication because the brain does not correctly detect the missed step.
That is why driving arguments become so painful.
The person may truly believe they are safe because the brain does not correctly update their current risk.
That is why financial arguments become so emotional.
The person may truly believe they paid the bills because the brain does not accurately track the breakdown.
You are asking the brain to inspect itself.
But the inspection system is already damaged.
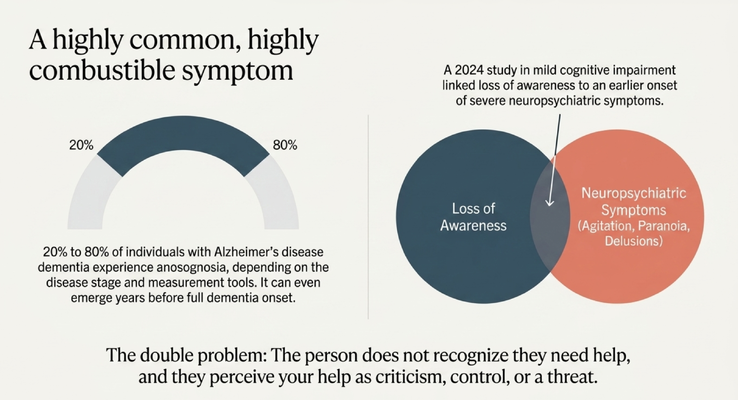
WHY THIS SYMPTOM BECOMES SO COMBUSTIBLE
Anosognosia is not rare.
It can affect a significant portion of people living with Alzheimer’s disease and other dementias, depending on disease stage and how it is measured.
But here is the part caregivers feel every day:
The person does not recognize they need help.
And when you offer help, they may experience that help as criticism, control, or threat.
That is the double problem.
You say:
“Mom, I need to help you with your medications.”
She hears:
“You think I am incapable.”
You say:
“Dad, I do not think you should drive today.”
He hears:
“You are taking away my independence.”
You say:
“I am going to help with the bills.”
They hear:
“You are trying to control my money.”
Now the person becomes fearful, angry, suspicious, ashamed, or defensive.
And the caregiver becomes frustrated, exhausted, and sometimes depressed because every attempt to help turns into a fight.
The caregiver is not trying to create conflict.
The caregiver is trying to prevent risk.
But the person living with dementia may not see the risk. They may only feel the loss of control.
That is why this symptom is so combustible inside the home.
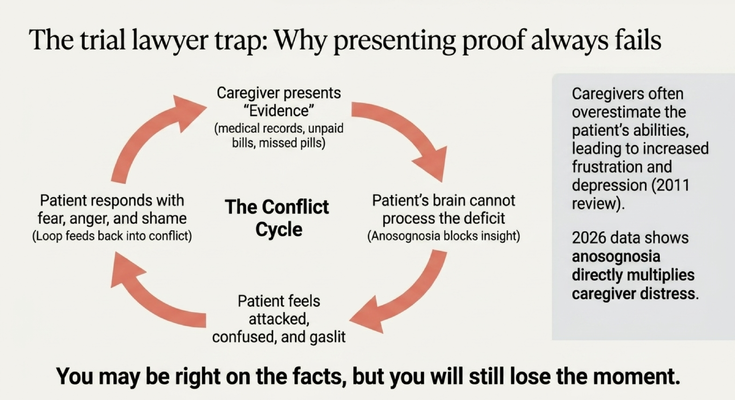
THE TRIAL LAWYER TRAP
One of the biggest mistakes caregivers make is what I call the trial lawyer trap.
The caregiver starts presenting evidence.
“Here are the unpaid bills.”
“Here are the medications you missed.”
“Here is the doctor’s note.”
“Here is the diagnosis.”
“Here are the car dents.”
“Here is what happened last week.”
And the caregiver is thinking:
“If I just show enough proof, they will finally understand.”
But with anosognosia, proof often fails.
Not because the caregiver is wrong.
The caregiver may be completely right on the facts.
But the person’s brain cannot process the deficit in the way the caregiver is asking.
So what happens?
The person feels attacked.
They feel confused.
They feel embarrassed.
They feel like the caregiver is gaslighting them.
They respond with fear, anger, shame, or suspicion.
Then the caregiver presents more evidence.
Then the person becomes more defensive.
And the cycle continues.
You may be right on the facts.
But you will still lose the moment.
That sentence is very important.
Because in dementia care, being factually correct is not always the same as being effective.
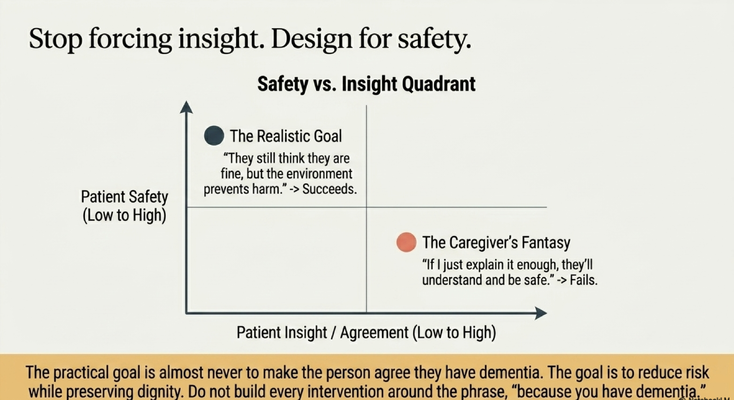
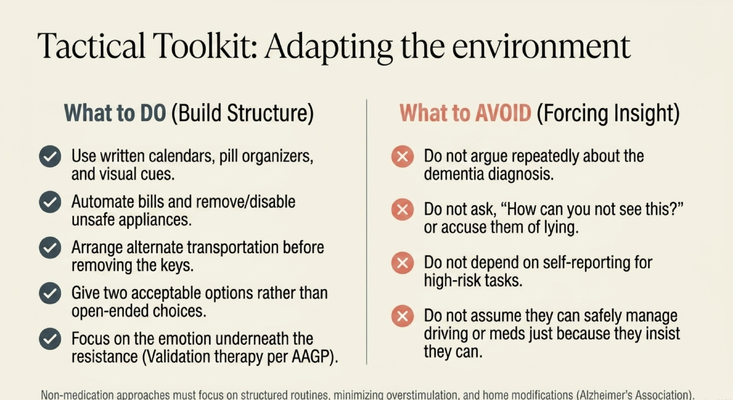
STOP FORCING INSIGHT. DESIGN FOR SAFETY.
The practical goal is usually not to make the person agree they have dementia.
The practical goal is to reduce risk while preserving dignity.
That is a very different mindset.
The caregiver’s fantasy is:
“If I just explain it enough, they will understand, agree, and be safe.”
But with anosognosia, that often fails.
The realistic goal is:
“They may still think they are fine, but I can change the environment so harm is less likely.”
That means we stop building every intervention around the phrase:
“Because you have dementia.”
Do not make every conversation a referendum on the diagnosis.
Do not keep saying:
“You cannot do this anymore because you have dementia.”
“You need help because you have dementia.”
“You are wrong because you have dementia.”
That front-door approach usually hits a locked door.
Instead, we design around safety.
If medications are being missed, we do not need to argue every day about whether the person forgot. We need a safer medication system.
If bills are unpaid, we do not need to fight every week about whether the person remembers. We need structure around finances.
If driving is unsafe, we do not need to win a courtroom argument at the kitchen table. We need a plan that reduces risk and preserves dignity as much as possible.
The goal is not forced agreement.
The goal is engineered safety.
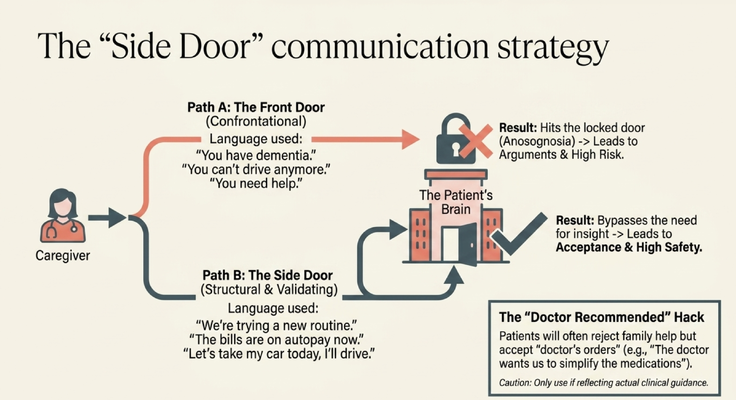
THE SIDE DOOR COMMUNICATION STRATEGY
This is where the side door becomes so important.
The front door is confrontational.
“Mom, you have dementia.”
“Dad, you cannot drive anymore.”
“You are not taking your pills correctly.”
“You need help.”
That language usually triggers defense.
The side door is structural and validating.
It bypasses the need for insight.
Instead of saying:
“Mom, you cannot manage the bills anymore because you have dementia,”
you might say:
“Mom, the bank has a new autopay option. It makes everything simpler, and we set it up so none of us have to worry about missing dates.”
Instead of saying:
“Dad, you cannot drive anymore,”
you might say:
“Let’s take my car today. I’ll drive.”
Or:
“The car is in the shop right now, so we are going to use another option.”
Instead of saying:
“You keep forgetting your medications,”
you might say:
“The doctor wants us to simplify the medication routine, so we are going to use this system.”
Now, I want to be clear.
Do not use “the doctor said” as a trick for things the doctor did not actually recommend.
But when there is real clinical guidance, it can help to shift the authority away from the family conflict.
Many people living with dementia will reject help from a spouse or adult child but accept something framed as a doctor’s recommendation.
The side door is not about manipulation.
It is about dignity.
It is about reducing unnecessary conflict.
It is about helping the person accept support without having to admit the thing their brain may not be able to recognize.
WHAT CAREGIVERS SHOULD REMEMBER
If you are caring for someone living with dementia, here is what I want you to remember.
When your loved one says, “There is nothing wrong with me,” do not automatically assume they are being stubborn.
They may have anosognosia.
Their brain may not be able to recognize the impairment.
That does not mean you ignore safety.
It means you stop trying to win the argument with facts.
If you keep presenting evidence and it keeps creating conflict, step back and ask:
“Am I trying to force insight?”
“Or am I designing for safety?”
Because those are different.
Forcing insight says:
“I need you to admit the problem before we can fix it.”
Designing for safety says:
“You may never fully see the problem, so I need to quietly build structure around the risk.”
That structure may involve medication systems, bill automation, transportation plans, home safety changes, caregiver supervision, simplified routines, written cues, or support from clinicians.
And please hear this clearly:
This is not about taking control for the sake of control.
This is about protecting the person you love while preserving as much dignity as possible.
Because dementia care is not only about memory.
It is about safety.
It is about identity.
It is about independence.
It is about grief.
It is about learning how to help someone who may not understand why help is needed.
That is hard.
And caregivers should not have to figure it out alone.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why the GUIDE Model matters.
GUIDE stands for Guiding an Improved Dementia Experience.
Through the GUIDE Model, eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Medicare-covered respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
Think about what that can mean for a caregiver dealing with anosognosia.
You may need help understanding why your loved one refuses support.
You may need someone to help you think through medication safety, driving concerns, or financial risk.
You may need help learning how to use the side door instead of the front door.
You may need a team to call when the situation escalates and you do not know what to do next.
Because this is not simple caregiving.
This is dementia caregiving.
And dementia caregiving requires education, structure, support, and a team around the family.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, anosognosia, caregiver communication, the GUIDE Model, and practical care strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, anosognosia, unsafe driving, medication errors, financial risk, behavioral escalation, caregiver burnout, safety concerns, and care planning should be discussed with qualified healthcare professionals. If symptoms are sudden, severe, dangerous, or medically concerning, seek immediate medical help.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health