DEMENTIA IS GRADUAL. DELIRIUM IS SUDDEN.
This distinction matters.
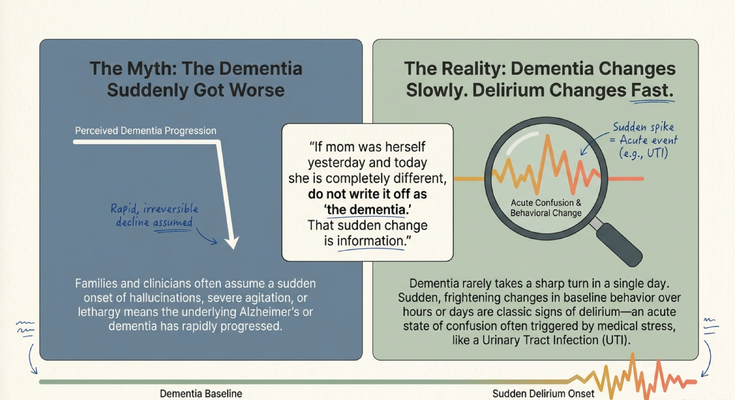
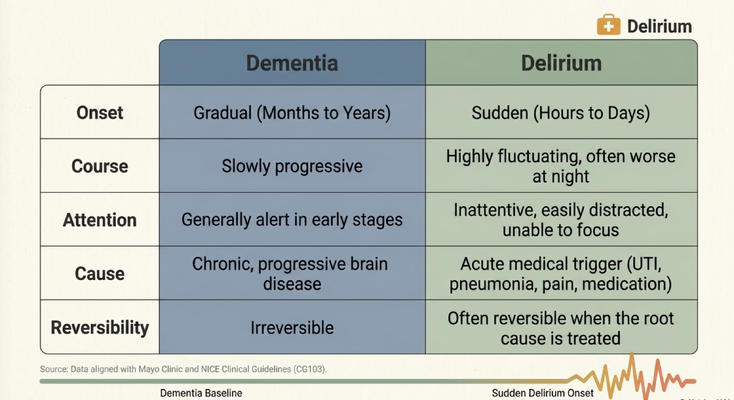
Dementia usually develops gradually. We are talking months to years. The person may repeat questions more often, miss appointments, struggle with bills, become less safe with driving, forget medications, or slowly lose independence.
Delirium is different.
Delirium can happen over hours to days. It can fluctuate dramatically. A person may seem relatively calm at breakfast, become extremely agitated in the afternoon, become lethargic by dinner, and then be severely confused or at fall risk overnight.
That up-and-down pattern is one of the major clues.
A caregiver may say, “But she was fine three hours ago.”
Exactly.
That does not rule out delirium. That may actually support it.
Delirium often fluctuates. It can be worse at night. It can look like sudden agitation, hallucinations, sleepiness, restlessness, inability to focus, or a sudden change in awareness.
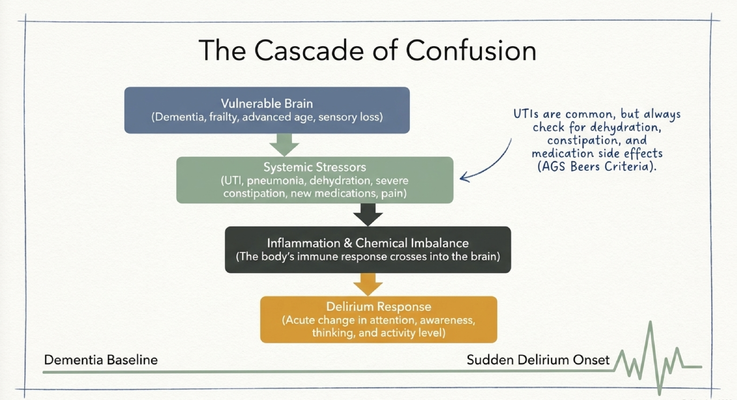
And the cause is often medical.
A UTI. Pneumonia. Pain. Medication changes. Dehydration. Constipation. Low sodium. Hospitalization. Surgery. Sleep disruption.
So if your loved one is suddenly different, do not jump straight to, “The dementia progressed.”
Ask, “Could this be delirium?”
THE 24-HOUR ROLLER COASTER
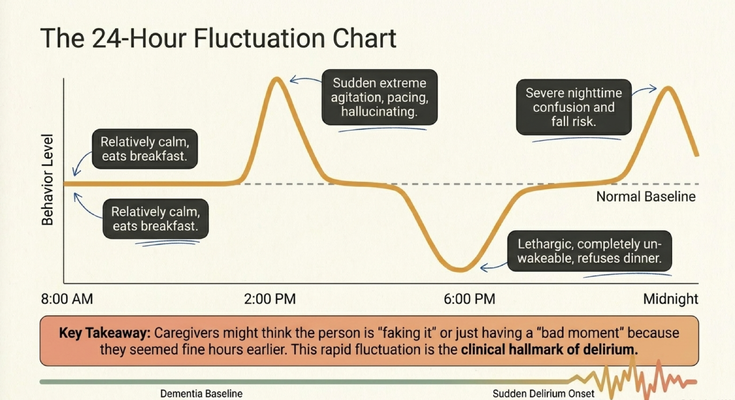
One of the most confusing parts of delirium is how much it can fluctuate in a single day.
Your loved one may wake up calm, eat breakfast, and seem close to normal.
Then two hours later, they may become extremely agitated, restless, pacing, suspicious, or hallucinating.
Then later, they may become lethargic, difficult to wake, or refuse dinner.
Then at night, they may become severely confused and at high risk for falls.
This is why caregivers sometimes think:
“Maybe they are faking it.”
Or:
“Maybe this is just a bad mood.”
Or:
“Maybe they are being difficult.”
But in dementia care, behavior is communication.
And rapid fluctuation can be the clinical hallmark of delirium.
The person is not choosing to be confusing. Their brain is responding to stress that the body cannot handle.
THE DEMENTIA BRAIN HAS LESS COGNITIVE RESERVE
Here is one way to think about it.
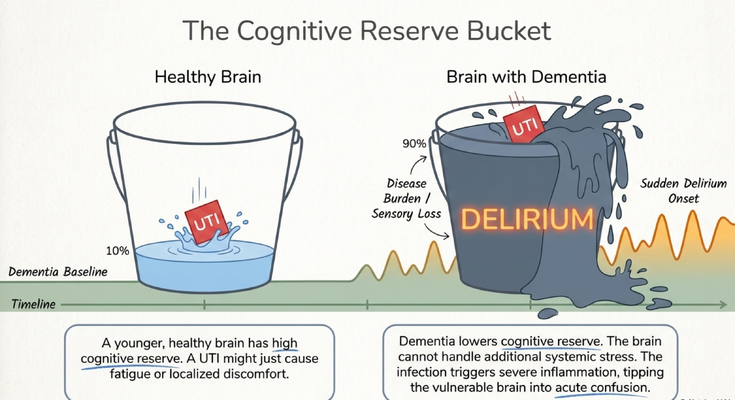
A younger, healthier brain may have more cognitive reserve. A UTI may cause burning, discomfort, fatigue, or fever, but the person can still say, “It burns when I urinate,” or “I think I have an infection.”
But a brain already affected by dementia has less reserve.
The bucket is already close to full.
Dementia, frailty, sensory loss, poor sleep, medications, and existing cognitive decline may already be placing stress on the system. Then you add a UTI, dehydration, constipation, pain, or a new medication.
Now the bucket overflows.
And what comes out?
Confusion.
Agitation.
Falls.
Sleepiness.
Hallucinations.
Paranoia.
Refusal to eat.
A sudden inability to walk or stand.
That is why a medical issue that might look mild in a younger adult can look dramatic in an older adult with dementia.
The brain does not have the same reserve to absorb the stress.
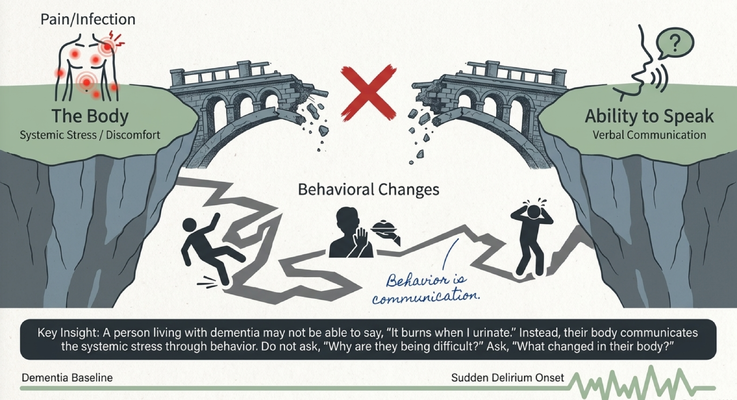
BEHAVIOR IS COMMUNICATION
I want caregivers to repeat this:
Behavior is communication.
A person living with dementia may not be able to say:
“It burns when I urinate.”
“I have lower back pain.”
“I feel dizzy.”
“I have not had a bowel movement.”
“My sodium is low.”
“This medication is making me feel strange.”
“I am dehydrated.”
“I am scared.”
Instead, the body communicates through behavior.
So when you see sudden behavior change, do not only ask:
“Why are they being difficult?”
Ask:
“What changed in their body?”
That shift can change the entire response.
If a caregiver assumes the person is “just being difficult,” they may correct, argue, sedate, or ignore the warning sign.
But if the caregiver understands behavior as communication, they become an advocate.
They start asking about infection, pain, dehydration, constipation, sleep, medication side effects, falls, and other acute triggers.
That is dementia care.
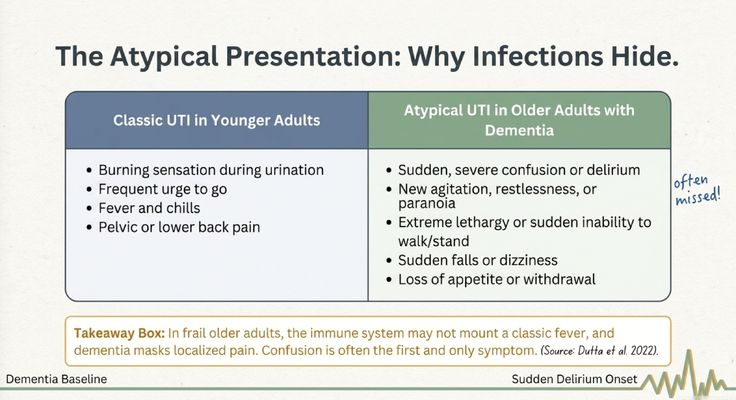
WHY UTIs CAN HIDE IN OLDER ADULTS WITH DEMENTIA
When most people think about a urinary tract infection, they think about burning with urination, frequent urge to go, fever, chills, pelvic pain, or lower back pain.
That is the classic picture.
But older adults with dementia may not present that way.
They may not be able to describe burning.
They may not report pain clearly.
They may already be wearing briefs, so changes in bathroom frequency may be missed.
They may not mount a strong fever.
They may not communicate symptoms in a way the family recognizes.
So what shows up first?
Sudden confusion.
New agitation.
Restlessness.
Paranoia.
Extreme lethargy.
Sudden inability to walk or stand.
Falls or dizziness.
Loss of appetite.
Withdrawal.
That is why UTIs can be missed.
The caregiver may say, “Mom does not have a fever. She did not say it burns. So it can’t be a UTI.”
But in dementia care, we have to be careful. The absence of a classic symptom does not always mean nothing is wrong.
Confusion may be the first and only obvious symptom.
DO NOT TREAT THE BEHAVIOR AND MISS THE CAUSE
Here is where we have to be very careful.
If a loved one suddenly becomes agitated, hallucinating, paranoid, or confused, some families immediately ask:
“Can we give something to calm them down?”
I understand why.
The situation is frightening. The caregiver is exhausted. The person may be unsafe. The house may feel like it is in crisis.
But if we only calm the behavior and miss the cause, we may create a bigger problem.
Imagine your loved one has a UTI. They become confused and agitated. Instead of asking why, the family assumes it is dementia progression and focuses only on sedation.
The agitation may quiet down temporarily.
But the infection is still there.
And if that infection progresses, it can spread and become much more serious.
This is why delirium matters.
Delirium is not just a behavior problem. It is often the brain’s response to a medical problem.
So the goal is not only to calm the person.
The goal is to find and treat the root cause.
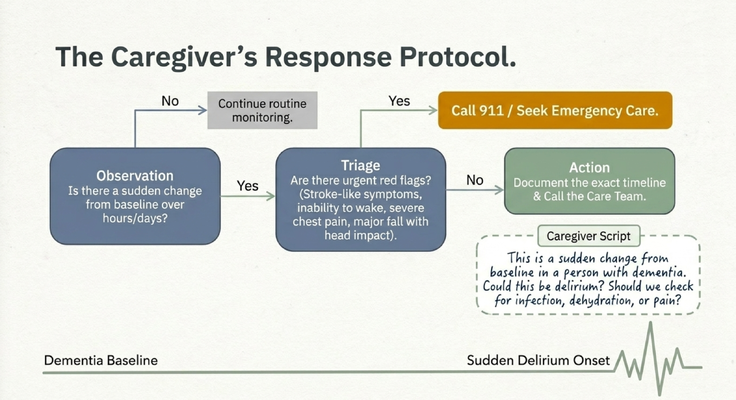
WHAT CAREGIVERS SHOULD DO FIRST
If your loved one suddenly changes, start with observation.
Is there a sudden change from baseline over hours or days?
If the answer is no, continue routine monitoring and keep watching for patterns.
If the answer is yes, then you triage.
Ask:
Is there weakness on one side of the body?
Is there slurred speech?
Are they unable to wake up?
Is there severe chest pain?
Was there a fall with head impact?
Are they severely confused in a way that feels dangerous?
If yes, call 911 or seek emergency care.
If there are no immediate emergency red flags, document the exact timeline and call the medical team.
And when you call, do not just say:
“She is confused.”
Give the doctor useful information.
Say:
“This is a sudden change from her baseline. Yesterday she could eat breakfast alone, and today she cannot hold a spoon. Could this be delirium? Should we check for infection, dehydration, constipation, pain, medication changes, or another cause?”
That is a much better call.
Good information in, better clinical guidance out.
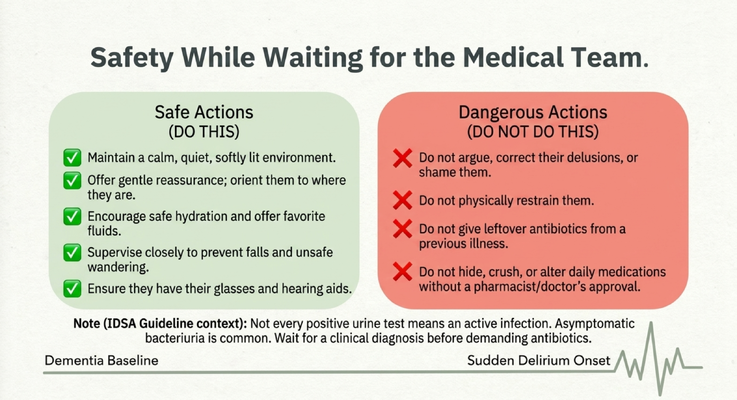
SAFETY WHILE WAITING FOR THE MEDICAL TEAM
While you are waiting for medical guidance, keep the environment calm and safe.
Use a quiet, softly lit room.
Offer gentle reassurance.
Orient the person to where they are.
Encourage safe hydration if they are able to drink safely.
Offer favorite fluids if appropriate.
Supervise closely to prevent falls or unsafe wandering.
Make sure they have their glasses, hearing aids, and dentures if they use them.
Those things matter.
If someone cannot hear, they may look more confused than they really are.
If they cannot see, they may misinterpret the environment.
If they are missing dentures, eating and communication may become harder.
Also, avoid dangerous actions.
Do not argue with them.
Do not correct delusions aggressively.
Do not shame them.
Do not physically restrain them unless there is an immediate safety emergency and trained help is involved.
Do not give leftover antibiotics from a previous illness.
Do not hide, crush, or change daily medications without medical or pharmacy guidance.
And one important point: not every positive urine test means there is an active infection requiring antibiotics. In older adults, asymptomatic bacteriuria can happen. That is why medical evaluation matters.
The goal is not to demand antibiotics automatically.
The goal is to describe the sudden change clearly and let the medical team evaluate what is actually going on.
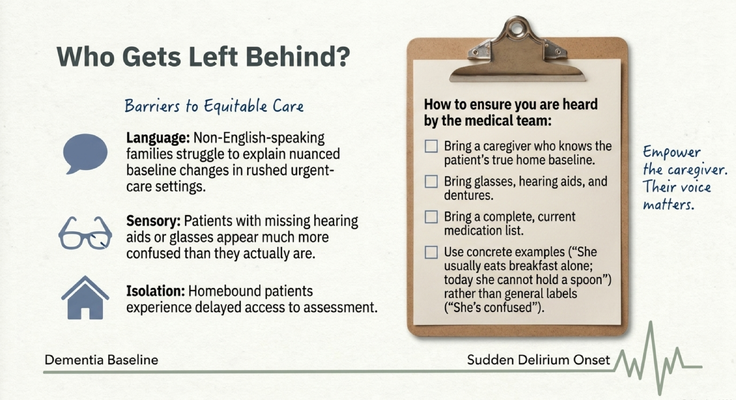
WHO GETS LEFT BEHIND
Some families face extra barriers when sudden confusion happens.
Non-English-speaking families may struggle to explain subtle baseline changes in a rushed urgent care or hospital setting.
Patients with missing hearing aids or glasses may appear much more confused than they actually are.
Homebound patients may experience delayed access to assessment.
Isolated caregivers may not know what information the medical team needs.
This is why caregiver advocacy matters.
If you are going to the hospital or calling the doctor, bring someone who knows the person’s real baseline.
Bring hearing aids, glasses, and dentures.
Bring a complete and current medication list.
Use concrete examples.
Not just, “She is confused.”
Say:
“She usually eats breakfast alone. Today she cannot hold a spoon.”
“She normally walks to the bathroom with a walker. Today she cannot stand.”
“She usually recognizes her daughter. Today she does not know who I am.”
“She normally sleeps at night. Last night she was awake, hallucinating, and trying to leave the house.”
Concrete examples help the medical team understand the seriousness of the change.
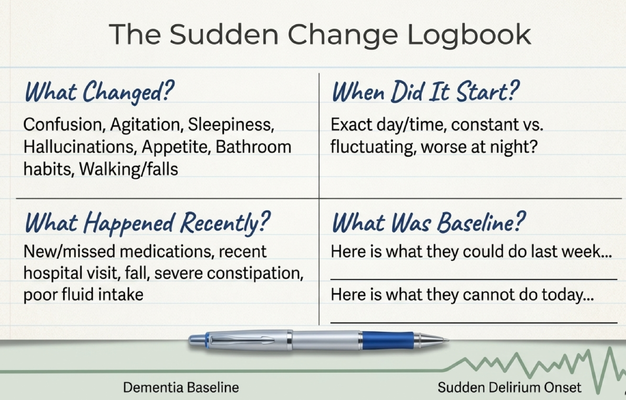
THE SUDDEN CHANGE LOGBOOK
One of the best tools caregivers can use is a simple logbook.
When something changes, write it down.
What changed?
Confusion, agitation, sleepiness, hallucinations, appetite, bathroom habits, walking, falls.
When did it start?
Exact day and time. Was it constant or fluctuating? Was it worse at night?
What happened recently?
New medication. Missed medication. Recent hospital visit. Fall. Severe constipation. Poor fluid intake. Poor sleep. New pain. New caregiver. Change in routine.
What was baseline?
What could they do last week?
What can they not do today?
That is the information clinicians need.
You do not have to use medical language.
You just need to tell the story clearly.
Because the caregiver knows the baseline.
And in delirium, baseline is everything.
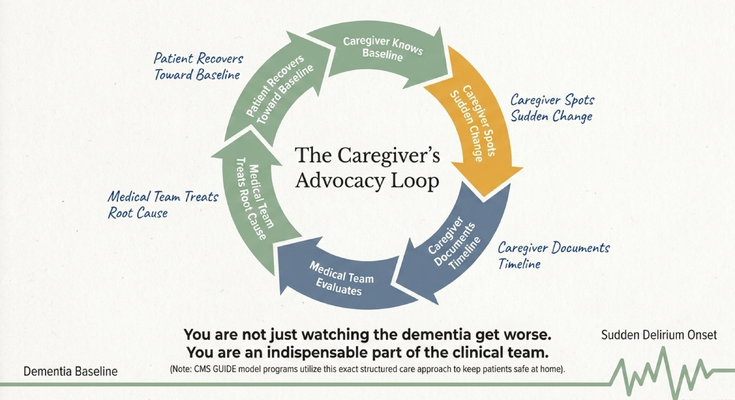
THE CAREGIVER IS PART OF THE CLINICAL TEAM
I want caregivers to hear this clearly:
You are not just watching the dementia get worse.
You are an indispensable part of the clinical team.
You know what your loved one looked like last week.
You know what changed today.
You know what they normally eat.
You know how they normally walk.
You know how they normally speak.
You know when something feels off.
That knowledge matters.
The caregiver spots the sudden change. The caregiver documents the timeline. The medical team evaluates. The medical team treats the root cause. The patient hopefully recovers toward baseline.
That is the advocacy loop.
And it starts with the caregiver saying:
“This is not their normal.”
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why caregivers should not have to navigate dementia alone.
Sudden confusion can be frightening. You may not know whether this is dementia progression, delirium, infection, dehydration, medication side effect, constipation, pain, or something else.
You may not know whether to call the doctor, go to urgent care, call 911, or keep monitoring.
You may not know what details to report.
That is why structured support matters.
Through the GUIDE Model — Guiding an Improved Dementia Experience — eligible families may receive dementia-care support through MedBetter Health.
MedBetterHealth.org is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because dementia care does not only happen in the clinic.
It happens in the kitchen.
It happens at 2 AM.
It happens when Mom suddenly cannot stand.
It happens when Dad is hallucinating.
It happens when the caregiver is asking:
“Is this dementia, or is something medically wrong?”
Families need someone to help them ask the right questions before a preventable crisis gets worse.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetterHealth.org currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about sudden confusion, delirium, UTIs, caregiver advocacy, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Sudden confusion, severe weakness, slurred speech, falls with head injury, chest pain, inability to wake, fever, medication concerns, suspected infection, dehydration, constipation, delirium, and safety risks should be discussed promptly with a qualified healthcare professional or emergency services when appropriate.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health