WHEN EGO ENTERS THE ROOM
I want to be very clear.
This is not about doctors versus nurse practitioners.
This is not about titles.
This is not about hierarchy.
I have worked with incredible physicians. I have worked with incredible nurse practitioners. I have worked with incredible physician assistants, nurses, social workers, care navigators, home care aides, therapists, and family caregivers.
And I have also seen people with every possible title handle conversations poorly.
The issue here is ego.
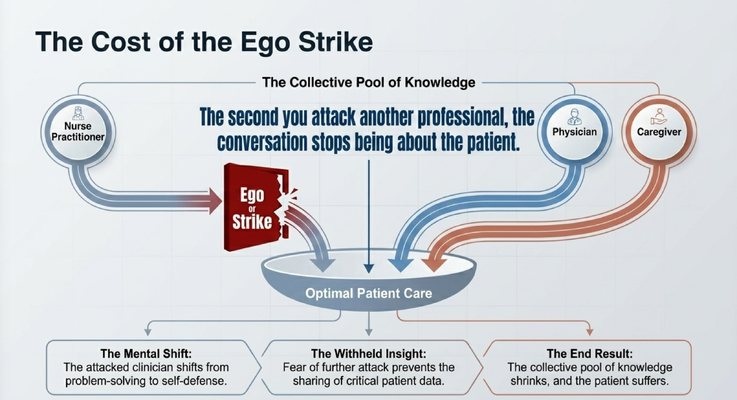
Because the second you attack another professional personally, the conversation stops being about the patient.
Now the person you attacked is no longer thinking, “How do we solve this problem?”
They are thinking:
“Why did you speak to me like that?”
“Do they think I’m not qualified?”
“Do I need to defend myself?”
“Is anything I say going to be attacked?”
And now you have changed the entire emotional frame of the conversation.
Instead of contributing to a shared pool of knowledge, people start protecting themselves.
They stop speaking freely.
They stop offering information.
They stop asking questions.
They stop saying the thing that might have helped the family.
And who suffers?
The patient.
The caregiver.
The family.
That is the real cost of ego in healthcare.
WHAT IS A CRUCIAL CONVERSATION?
There is a book I recommend often called Crucial Conversations.
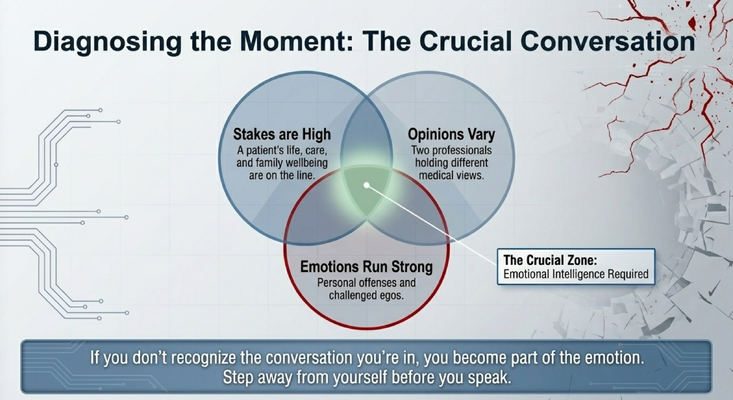
The basic idea is simple: a crucial conversation has three ingredients.
The stakes are high.
Opinions vary.
Emotions run strong.
That is dementia care every single day.
Should Mom stay at home or move into assisted living?
Should Dad continue driving?
Should we start medication?
Should we stop medication?
Is this delirium, dementia progression, depression, pain, infection, or medication side effect?
Is the caregiver still able to do this?
Is the home still safe?
Does the family need more support?
These are not casual conversations.
They are high-stakes conversations.
A patient’s life may be affected. A caregiver’s health may be affected. Family relationships may be affected. Safety may be affected. Finances may be affected.
And when people disagree, emotions rise quickly.
So the first thing you have to do is recognize the moment you are in.
You have to step outside yourself and say:
“I am in a crucial conversation.”
If you do not recognize that, you become part of the emotion.
You react instead of leading.
You defend instead of listening.
You attack instead of asking.
And the patient gets pushed to the side.
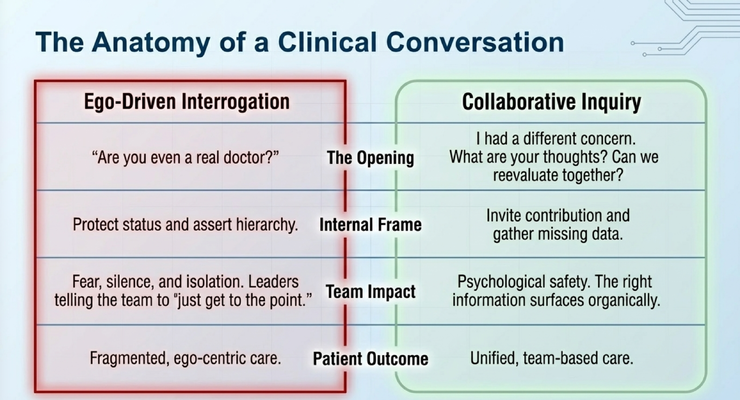
THE WRONG OPENING VERSUS THE RIGHT OPENING
Let’s look at the difference.
The wrong opening is:
“Are you even a real doctor?”
What does that do?
It protects status.
It asserts hierarchy.
It makes the other person defensive.
It creates fear.
It tells the team, “Be careful what you say around me.”
And the outcome is fragmented, ego-centered care.
Now compare that to a better opening:
“I had a different concern. What are your thoughts? Can we reevaluate this together?”
That is a completely different conversation.
Now you are not attacking the person. You are addressing the clinical issue.
You are inviting contribution.
You are gathering missing data.
You are allowing the other person to bring what they know into the conversation.
You are building psychological safety.
And psychological safety is not soft.
It is not a corporate buzzword.
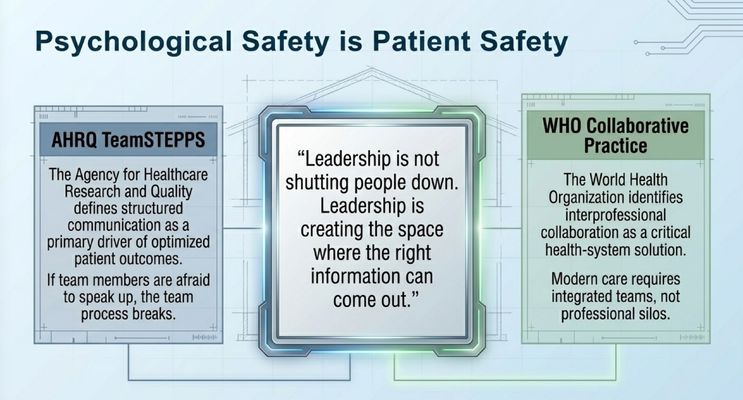
In healthcare, psychological safety is patient safety.
Because if people are afraid to speak, the right information may never come out.
PSYCHOLOGICAL SAFETY IS PATIENT SAFETY
Leadership is not shutting people down.
Leadership is creating the space where the right information can come out.
That applies to doctors.
That applies to nurse practitioners.
That applies to administrators.
That applies to home care agency owners.
That applies to family caregivers.
If people around you are afraid to speak honestly, your care process breaks.
If a nurse is afraid to question something, you may miss a problem.
If a caregiver is afraid to say, “I cannot do this anymore,” the family may wait until collapse.
If a home care aide is afraid to report a change in behavior, the team may miss infection, pain, or delirium.
If the nurse practitioner is attacked for giving input, the next time they may stay quiet.
And silence is dangerous in dementia care.
Why?
Because dementia care is complicated.
The person living with dementia may not be able to explain what they feel. They may not say, “I am in pain.” They may not say, “I am scared.” They may not say, “This medication is making me dizzy.” They may not say, “I cannot swallow.” They may not say, “I am lonely.”
So we need the people around them to speak.
We need the caregiver’s observations.
We need the home care worker’s pattern recognition.
We need the clinician’s judgment.
We need the care navigator’s coordination.
We need the family’s history.
Nobody has the whole picture alone.
THE CAREGIVER IS NOT ON THE SIDE
Here is where this becomes especially important in dementia care.
The caregiver is not on the side.
The caregiver is part of the care plan.
In a hospital or clinic, people sometimes talk about the patient as if the caregiver is only a visitor. But in dementia care, the caregiver is often the person holding the entire care system together.
They know what happens at 7 PM.
They know when the hallucinations start.
They know when bathing becomes impossible.
They know when medications are being refused.
They know when the person is wandering.
They know when the person is eating less.
They know when sleep has collapsed.
They know when something feels different.
That information is clinical information.
And if the caregiver does not feel safe saying it, the team misses the truth.
High-stakes communication does not only happen between clinicians.
It happens between clinician and family.
It happens between family and patient.
It happens in the home, in the dark, at 10 PM, when there is no medical team standing in the room.
That is why communication matters so much.
In dementia care, the way we talk is not separate from the care plan.
It is part of the care plan.

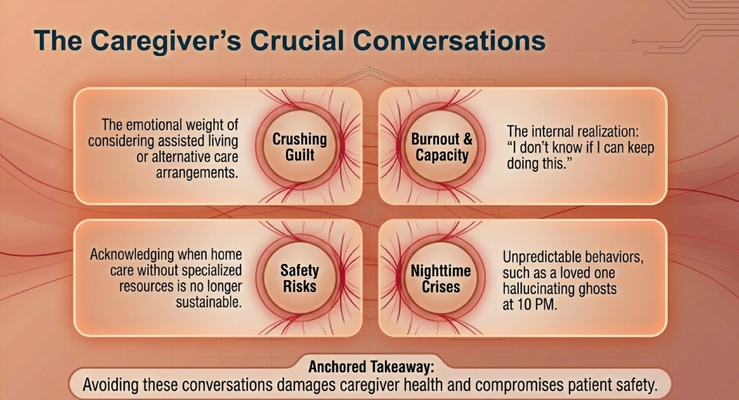
THE CAREGIVER’S CRUCIAL CONVERSATIONS
Caregivers have crucial conversations too.
They may not use that language, but they live it every day.
They have to ask:
“Can I still keep Mom at home?”
“Am I putting Dad at risk if I leave him alone?”
“Do we need assisted living?”
“Do we need more help?”
“Can I keep doing this?”
“Am I failing if I say I need support?”
These are incredibly painful questions.
There is guilt.
There is burnout.
There are safety risks.
There are nighttime crises.
There are unpredictable behaviors.
There are moments where the caregiver looks in the mirror and thinks, “I don’t know if I can keep doing this.”
And too often, caregivers avoid these conversations because they feel ashamed.
They think needing help means they are giving up.
They think discussing assisted living means they are abandoning their loved one.
They think saying, “I am exhausted,” makes them weak.
It does not.
It makes them human.
Avoiding these conversations does not protect the caregiver.
It damages the caregiver’s health.
And eventually, it can compromise patient safety.
So when a caregiver says, “I cannot do this alone anymore,” the response should not be judgment.
The response should be:
“Let’s talk about what support this family needs.”
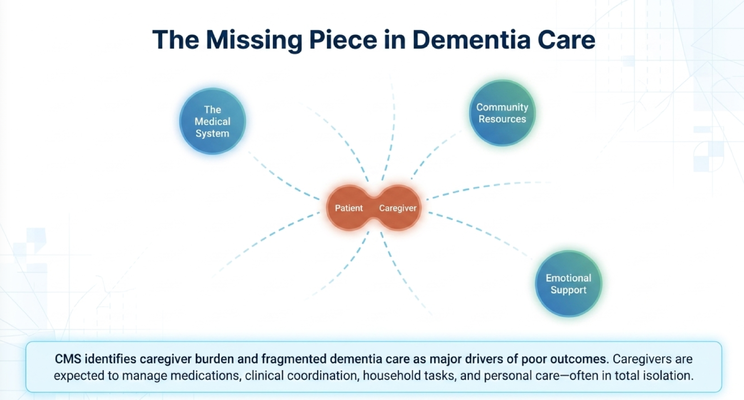
THE MISSING PIECE IN DEMENTIA CARE
One of the biggest problems in dementia care is fragmentation.
The medical system is over here.
Community resources are over there.
Emotional support is somewhere else.
And in the middle, you have the patient and caregiver trying to connect all the dots alone.
That is not fair.
A caregiver may be managing medications, appointments, transportation, bathing, meals, sleep disruption, hallucinations, wandering risk, insurance questions, family conflict, and their own health at the same time.
And then we wonder why caregivers burn out.
The problem is not that caregivers are not strong enough.
The problem is that we keep asking caregivers to function as the entire care system by themselves.
That is not sustainable.
Families need coordinated care.
They need a system that recognizes that dementia does not stay inside the doctor’s office.
It follows the family home.
It shows up in the kitchen.
It shows up in the bathroom.
It shows up when the caregiver tries to leave the house.
It shows up when Mom starts seeing things at 10 PM.
It shows up when Dad refuses medication.
It shows up when the home care aide says, “I cannot manage this.”
That is where support has to exist.
WHERE THE GUIDE MODEL FITS IN
This is exactly why the GUIDE Model matters.
The GUIDE Model — Guiding an Improved Dementia Experience — was created by CMS and Medicare to support people living with dementia and the caregivers caring for them at home.
MedBetter Health is proud to participate in this CMS-selected dementia care model.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 support line for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because the caregiver should not have to figure out every crisis alone.
Imagine it is 10 PM.
Mom is seeing something that is not there.
The caregiver is scared.
They are thinking:
“Is this an emergency?”
“Do I call 911?”
“Do I try to redirect?”
“Is this dementia?”
“Is this delirium?”
“What do I say right now?”
That is a crucial conversation too.
And in that moment, the caregiver needs more than a pamphlet.
They need someone who can help them walk through the situation step by step.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, caregiver support, communication, and practical care strategies by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Medical decisions, dementia symptoms, medication concerns, safety issues, caregiver burnout, and care transitions should be discussed with qualified healthcare professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health