FAMILY CONFLICT IS COMMON IN DEMENTIA CARE
Let’s start with the reality.
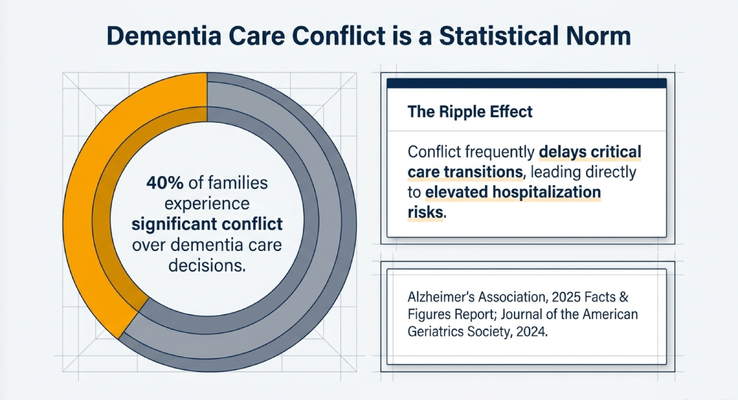
Family conflict in dementia care is not unusual.
The presentation highlighted that 40% of families experience significant conflict over dementia care decisions. That is 4 out of 10 families that we know of.
And honestly, from what I see in real life, I would not be surprised if many caregivers feel like that number should be even higher.
Why?
Because dementia does not affect only the person diagnosed.
It affects the entire family system.
One sibling may see the decline every day because they live nearby.
Another sibling may visit once a month and say, “She looks fine to me.”
One person may be managing medications, meals, appointments, bathing, transportation, finances, and nighttime confusion.
Another person may only hear updates by phone and think everyone is exaggerating.
One person may say, “Mom needs home care.”
Another may say, “We do not need strangers in the house.”
One person may say, “Dad should not be driving.”
Another may say, “You are taking away his independence.”
And suddenly the family is not only dealing with dementia.
They are dealing with disagreement, guilt, denial, resentment, fear, and old family dynamics that dementia brings back to the surface.
WHEN DISAGREEMENT BECOMES DANGEROUS
Family disagreement is not just emotionally exhausting.
It can create real risk.
Let me give you an example.
Mom is declining. Physical therapy comes into the home and says, “She really needs a walker. She is at high risk for a fall.”
One brother says, “We should probably listen to the physical therapist.”
Mom says, “No, I do not want a walker.”
Another brother says, “She is fine. You are overreacting. The therapist just wants to give advice. Stop treating Mom like she is helpless.”
Now there is conflict.
No decision is made.
No walker.
No home safety changes.
No consensus.
Then Mom falls.
Now the family is in the hospital having the same conversation they avoided at home.
Or take driving.
Dad is still driving. One child says, “I rode with him. He seemed okay.”
Another child says, “I am seeing scratches on the car. He has gotten lost. I do not think this is safe anymore.”
Then the accusations start.
“You are always overprotective.”
“You are babying him.”
“You are trying to control him.”
“You are taking away his freedom.”
And while the family is arguing, Dad is still driving.
God forbid he gets into an accident. Now the consequences may affect not only Dad, but other people on the road.
That is the danger.
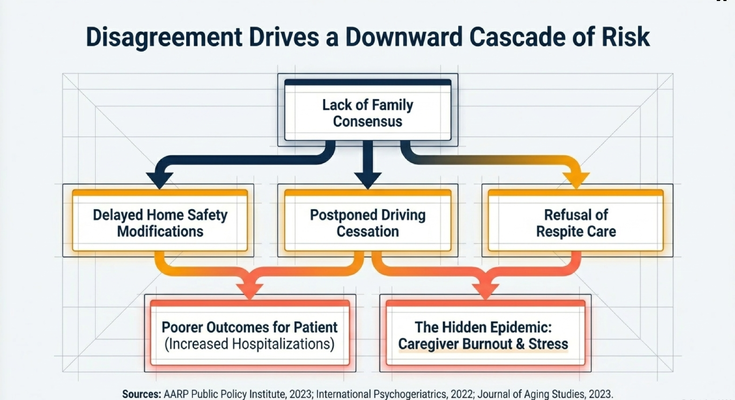
In dementia care, delayed decisions can become dangerous decisions.
Home safety gets delayed.
Driving conversations get delayed.
Respite gets delayed.
Legal planning gets delayed.
Care transitions get delayed.
And when action is delayed, the person living with dementia and the caregiver both carry more risk.
THE CONVERSATIONS YOU SHOULD NOT WAIT TO HAVE
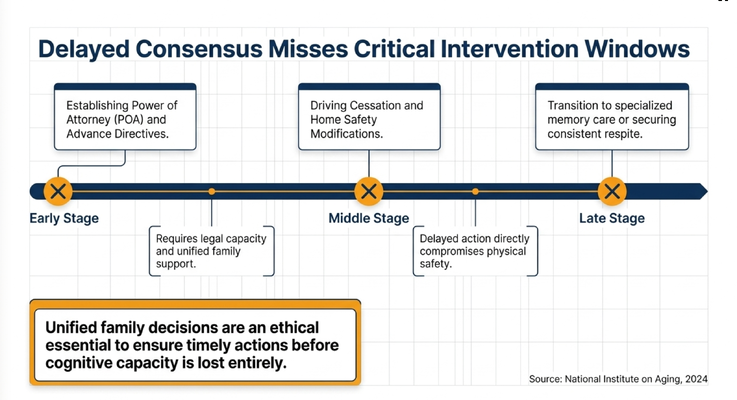
One of the most important parts of this topic is timing.
Some conversations require the person living with dementia to still have enough capacity to participate.
Power of attorney.
Healthcare proxy.
Advance directives.
Goals of care.
Driving preferences.
Future care setting.
Who should make decisions if the person cannot?
These are not conversations to wait on until the disease is severe.
If Mom is still early enough in the disease process and can participate, that is the time to ask:
“Mom, if there ever comes a time when you cannot make medical decisions, who do you trust to make those decisions for you?”
“Dad, if there ever comes a time when driving is not safe, how would you want us to handle that?”
“If your health changes, what kind of care would you want?”
“Would you want CPR or intubation in certain circumstances?”
“Who should be your healthcare proxy?”
“Who should handle finances if you cannot?”
I know these conversations are uncomfortable.
But compare that to the alternative.
Mom collapses at home. 911 comes. She is intubated. She is resuscitated. Now five siblings are standing in a hospital hallway arguing about what she would have wanted.
One person says, “She would never want this.”
Another says, “You are trying to kill Mom.”
Another says, “We need to speak with our rabbi first.”
Another says, “I talked to her last year and she told me something different.”
I have seen this as a doctor.
And I am telling you, that is not the moment you want to discover the family never had the conversation.
It is better to have the difficult conversation before the difficult situation.
WHY FAMILIES GET STUCK
When a family is fighting, the surface argument is usually not the whole story.
It may look like the family is arguing about a walker, driving, home care, assisted living, respite, or who should make decisions.
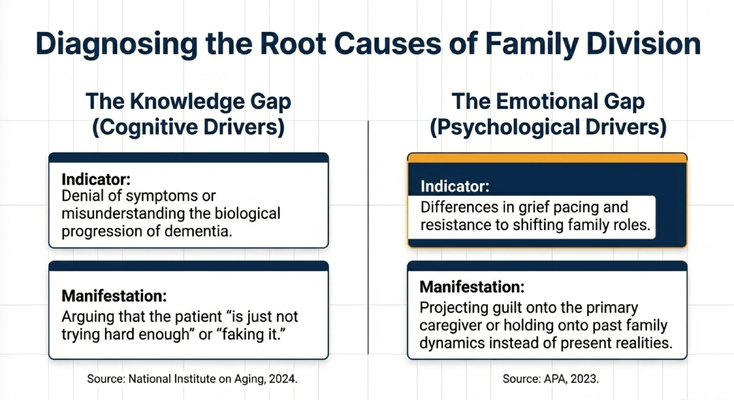
But underneath, there are usually two major gaps.
The first is the knowledge gap.
This is when family members do not understand dementia progression.
One sibling may say, “Dad is just not trying hard enough.”
Another may say, “Mom is faking it.”
Another may think, “If we push her, she will remember.”
But dementia is not a motivation problem.
It is a brain disease.
If a loved one cannot sequence bathing, cannot manage medications, cannot judge driving risk, cannot safely walk without support, or cannot understand why a walker matters, that may not be stubbornness.
That may be cognitive decline.
The second is the emotional gap.
This is grief.
This is denial.
This is guilt.
This is the pain of watching a parent change.
This is the adult child who cannot accept that Mom is no longer the person who raised them.
This is the sibling who lives far away and does not want to believe things are as bad as they are.
This is the caregiver who is burned out but feels guilty asking for help.
This is the family member who projects old family issues onto the current care crisis.
So before we judge the conflict, we have to diagnose it.
Is this a knowledge gap?
Is this an emotional gap?
Or is it both?
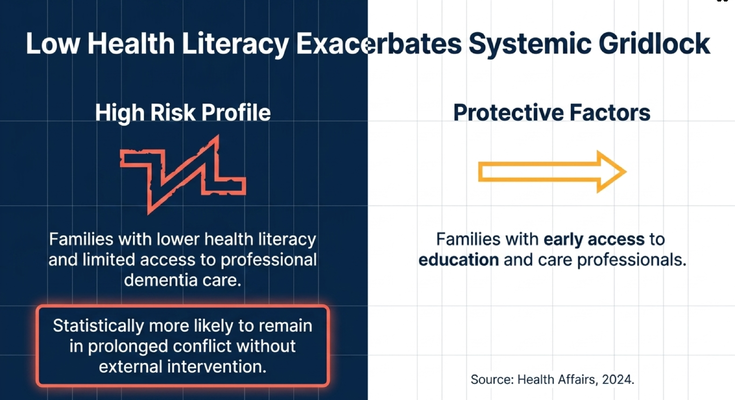
LOW HEALTH LITERACY MAKES EVERYTHING HARDER
Another issue is health literacy.
If families do not understand dementia, they are more likely to remain stuck in arguments.
Why?
Because without a shared understanding of the disease, everyone argues from emotion.
One person says, “She is fine.”
Another says, “She is not safe.”
One person says, “He just needs to try harder.”
Another says, “This is the dementia.”
One person says, “We should wait.”
Another says, “Waiting is dangerous.”
If nobody has an objective framework, the loudest voice often wins.
But the loudest voice is not always the safest voice.
Families need education.
They need credible information.
They need someone who can explain what dementia does to memory, judgment, walking, safety, driving, medication management, behavior, communication, and caregiver burden.
That education matters because it changes the conversation.
Instead of arguing, “What do I want?”
The family can begin asking:
“What does Mom need?”
“What is safest right now?”
“What is the caregiver actually capable of sustaining?”
“What decision cannot wait?”
That shift matters.
THE THREE THINGS FAMILIES NEED TO DO
So what do we do?
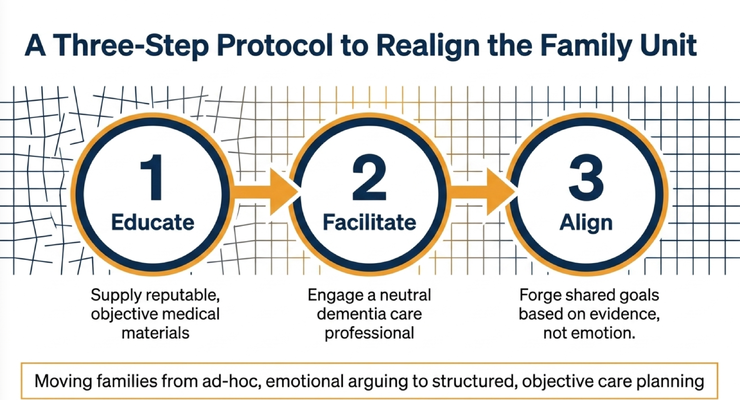
We move the family from emotional arguing to structured care planning.
I want families to think about three steps.
Educate.
Facilitate.
Align.
Step one: educate.
Before the family tries to make big decisions, everyone needs the same basic information. What stage is the person in? What has changed? What does the doctor say? What does the primary caregiver see every day? What are the safety risks? What decisions are urgent?
If one person understands dementia and the rest of the family does not, every conversation becomes lopsided.
Step two: facilitate.
If the family has been arguing for years, do not expect one emotional phone call to fix everything.
Bring in a neutral professional when possible. A dementia care professional, care navigator, social worker, physician, nurse practitioner, elder care mediator, or another qualified guide can help keep the conversation focused.
The facilitator’s job is not to pick sides.
The job is to bring the conversation back to the person living with dementia, the caregiver’s capacity, and the actual care needs.
Step three: align.
Alignment does not mean everyone gets exactly what they want.
It means the family agrees on shared goals based on safety, dignity, and the clinical reality.
Not:
“I want Mom to stay home forever no matter what.”
Not:
“I do not want strangers in the house.”
Not:
“I refuse respite because I feel guilty.”
The better question is:
“What is safest for Mom right now?”
“What support does the caregiver need right now?”
“What decision has to be made before the next crisis?”
That is how families move from fighting to planning.
RESPITE IS NOT A FAILURE
I want to stop on one example because it comes up constantly.
Respite.
Many caregivers say:
“No, I do not need respite.”
“I am okay.”
“I can handle it.”
“Let’s just see what happens.”
But then what happens?
The caregiver gets sick.
The caregiver becomes depressed.
The caregiver stops sleeping.
The caregiver misses their own doctor’s appointments.
The caregiver becomes the entire care system, and eventually the care system breaks.
I always use the airplane example.
When the oxygen masks come down, what do the flight attendants tell you?
Put the mask on yourself first before helping the person next to you.
Why?
Because if you cannot breathe, you cannot help anyone else.
Dementia caregiving works the same way.
If you are the caregiver and you never put the mask on yourself, eventually you will not be able to take care of the person living with dementia.
Respite is not abandonment.
Respite is oxygen.
It is what allows care to continue.
And sometimes the family conflict is that everyone agrees Mom needs care, but nobody wants to admit the caregiver needs care too.
That has to change.
THE FAMILY MEETING NEEDS STRUCTURE
If your family needs to have this conversation, do not wing it.
Structure matters.
Before the meeting, gather the facts.
What changed in the last 3 months?
What safety issues have happened?
Any falls?
Any medication errors?
Any wandering?
Any driving concerns?
Any missed appointments?
Any caregiver health concerns?
Any doctor recommendations?
Any home care or therapy recommendations?
Then set ground rules.
No personal attacks.
No old grievances.
No blaming the primary caregiver.
No interrupting.
No pretending this is only about what one person wants.
The meeting is about care planning.
Then define the priorities.
Safety first.
Legal documents.
Medical needs.
Caregiver capacity.
Driving.
Home safety.
Respite.
Future care setting.
Then assign roles.
One person may handle finances.
Another may schedule appointments.
Another may help with respite.
Another may research home care.
Another may help with legal documents.
Roles should be based on capacity, not guilt.
The person who lives closest should not automatically be expected to carry everything.
And the person with the loudest opinion should not automatically control the plan.
The family has to move from emotion to responsibility.
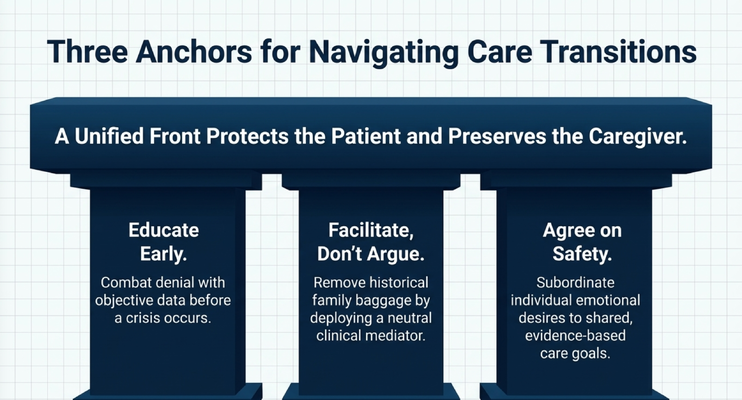
THE THREE ANCHORS
If you remember nothing else from this issue, remember these three anchors.
Educate early.
Do not wait until crisis. Combat denial with objective information before decisions become emergencies.
Facilitate, do not argue.
If the family is stuck in old patterns, bring in someone neutral. Remove historical baggage from the care conversation.
Agree on safety.
Individual emotions matter, but they cannot override shared, evidence-based care goals.
A unified family protects the person living with dementia.
And it preserves the caregiver.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why caregivers should not have to navigate dementia care alone.
Family conflict is not just emotional. It affects care decisions, safety, caregiver health, and the timing of critical interventions.
Through the GUIDE Model — Guiding an Improved Dementia Experience — eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because sometimes the family needs someone to help organize the chaos.
Someone to help ask:
What stage are we in?
What safety risks are urgent?
What decisions need to happen now?
What does the caregiver need?
What should the family prepare for next?
Who is responsible for which part of the plan?
That is not a luxury in dementia care.
That is the difference between crisis-driven decision-making and structured support.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about family conflict, dementia care planning, caregiver support, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Legal planning, power of attorney, healthcare proxy, advance directives, driving safety, care transitions, and medical decisions should be discussed with qualified professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health