I took a red-eye flight, landed around 9 AM, and I was tired. But I was also energized.
Why?
Because I had just spent several days with more than 1,000 Alzheimer’s advocates from across the country at the 2026 AIM Advocacy Forum.
Picture this: more than 1,000 people wearing purple, gathered in Washington, D.C., walking through Capitol Hill, meeting with members of Congress, sitting with House and Senate offices, and telling real stories about what Alzheimer’s disease and dementia do to families.

I had my purple suit on. I had my purple sash on. And I was there with advocates from Florida and across the country because this disease is not just a medical issue.
It is a family issue.
It is a caregiver issue.
It is a healthcare system issue.
It is a policy issue.
And if we want dementia care to change, we cannot only talk about it inside exam rooms. We have to talk about it where decisions are made.
My name is Dr. Erik Ilyayev. I’m a dementia care physician, a board member of the South Florida Alzheimer's Association® , and the CEO of MedBetterHealth.org — one of the organizations selected by Medicare to participate in a groundbreaking new program designed to change how America cares for people living with dementia.
In this issue, I want to share why this advocacy trip mattered, what we were fighting for, and why early detection, clinician education, caregiver support, and federal policy all connect back to the same question:
How do we give families a better path before the crisis happens?
WHY WE WENT TO WASHINGTON
The Alzheimer’s Association and the Alzheimer’s Impact Movement brought advocates together in Washington because families need more than awareness.
They need action.
At the forum, advocates from all 50 states came together to speak with federal policymakers about the realities of Alzheimer’s disease and other dementias. We went to Capitol Hill. We met with congressional offices. We talked about screening, prevention, provider education, and the need to support families before they are drowning.
For Florida, we met with teams connected to Senator Rick Scott, Senator Ashley Moody, and Congresswoman Debbie Wasserman Schultz’s office. I was there with an incredible group of advocates, including John Strader, Tracy Page from the Alzheimer’s Association in South Florida, and my good friend Josh Lawrence.
And that was just one small part of the room.
There were caregivers there. Physicians. Advocates. Families. People who lost someone to Alzheimer’s. People currently caring for someone. People who have dedicated their lives to making sure the next family does not go through this alone.
And I want you to understand something.
These people were volunteers.
They left their homes. They left their families. They gave their time. They traveled to Washington because this disease has touched their lives, and they want the system to change.
There were a lot of emotional stories.
There were a lot of tissues.
Because when you hear caregiver after caregiver explain what this disease took from their family, you realize something very quickly:
Alzheimer’s is not just memory loss.
It is identity loss. Independence loss. Family stress. Financial pressure. Caregiver exhaustion. Grief before death. And too often, a diagnosis that comes too late.
THE “MAMMOGRAM MOMENT” FOR ALZHEIMER’S DISEASE
One of the major issues we discussed was early detection.
I want you to think about breast cancer screening for a moment.
Years ago, many women were not getting regular screening. By the time breast cancer was found, it was often much later than it should have been. Then screening became part of the public conversation. Mammograms became a standard tool. Earlier detection changed the way families and doctors approached the disease.
Alzheimer’s disease is having a similar moment.
For years, families were often told some version of:
“Let’s wait and see.”
“It might just be normal aging.”
“Come back when it gets worse.”
But by the time the person and family realize something is truly wrong, the disease may already be moderate or severe.
And that matters.
Because timing matters.
If someone is in the mild cognitive impairment stage or early Alzheimer’s disease stage, that is a very different moment than when they are already in moderate or severe dementia. The family can plan earlier. The person can participate in decisions. Legal and financial planning can happen while the person still has more capacity. Safety decisions can be made before crisis. And for some patients, newer treatment options may only be considered in earlier stages.
That is why early detection matters.
Not because a test magically solves everything.
But because knowing earlier gives families time.
Time to plan.
Time to prepare.
Time to ask the right questions.
Time to understand what is happening before the disease takes away the person’s ability to participate in their own future.
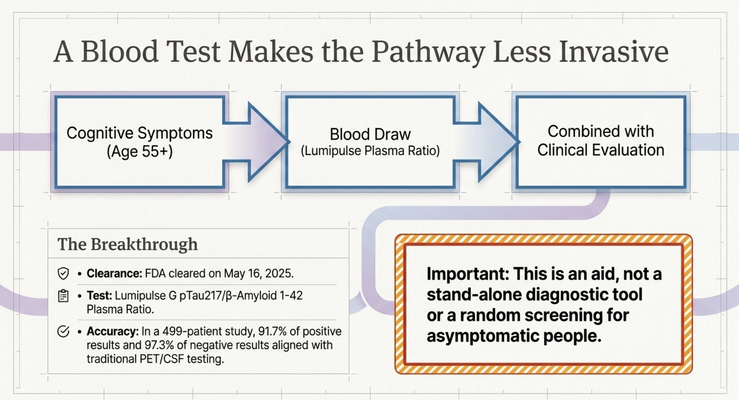
BLOOD TESTING AND ACCESS
This is where blood-based testing becomes so important.
The science is moving quickly. Blood tests for Alzheimer’s disease biomarkers are now part of the national conversation in a way they were not years ago. The FDA cleared the first blood test to help diagnose Alzheimer’s disease in 2025, designed for people 55 and older who already have signs and symptoms of cognitive decline.
That is a major step.
Because historically, confirming Alzheimer’s disease biology often required specialized testing, like PET scans or spinal fluid testing. Those are not easy for every family to access. They can be expensive, invasive, geographically limited, or difficult to coordinate.
A blood test is different.
It does not replace a full clinical evaluation. It does not mean every person without symptoms should start testing themselves randomly. It still has to be interpreted by clinicians alongside history, cognitive testing, function, imaging, and the full medical picture.
But it can make the pathway easier.
And that is the point.
Families should not have to jump through endless hoops just to understand what is happening.
If we believe early detection matters, then access to early detection matters too.
EARLY DETECTION IS NOT ONLY ABOUT MEDICATION
Now, some people may hear this and say:
“Dr. Erik, what is the point of knowing early if there is no cure?”
I understand that question.
But early detection is not only about medication.
It is about planning.
It is about safety.
It is about family decision-making.
It is about the person living with memory changes having a voice while they still can.
It is about driving decisions, medication management, finances, powers of attorney, advance directives, home safety, caregiving support, and knowing what kind of care the person would want later.
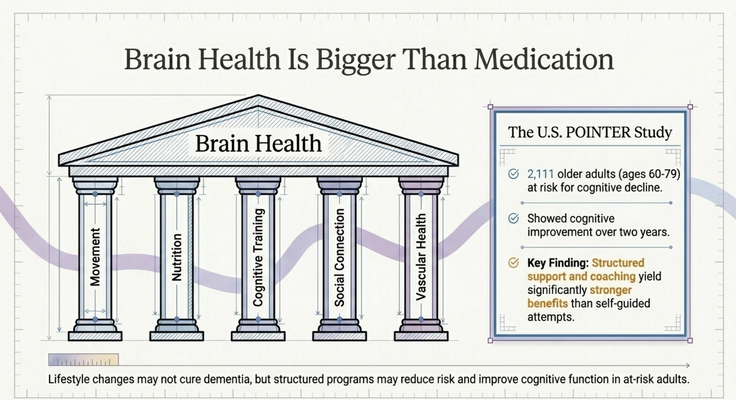
It is also about lifestyle.
At the forum, I talked about the U.S. POINTER study, which was spearheaded by the Alzheimer’s Association. That study focused on lifestyle interventions like physical activity, nutrition, cognitive exercises, sleep, social connection, and vascular risk management.
And this is important because families often think prevention means only medication.
It does not.
Brain health is bigger than that.
Exercise matters.
Nutrition matters.
Sleep matters.
Cognitive engagement matters.
Social connection matters.
Managing blood pressure, diabetes, cholesterol, hearing loss, and other risk factors matters.
No lifestyle plan guarantees that someone will never develop dementia. But the research is telling us that structured lifestyle interventions can support cognitive health and may slow decline in people at risk.
So early detection gives us a window.
A window to plan.
A window to act.
A window to build support before everything becomes reactive.
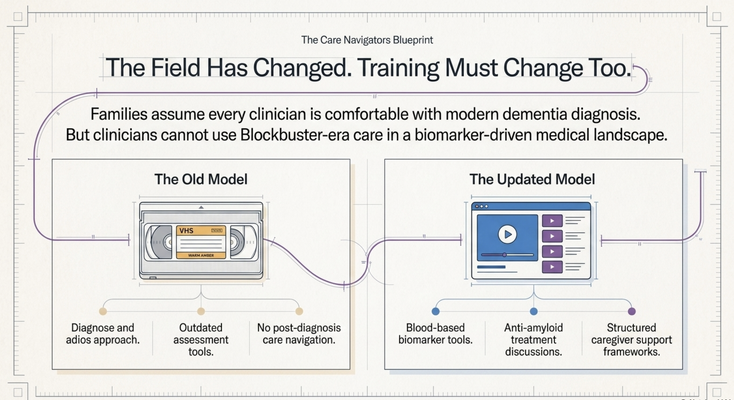
THE ADAPT ACT AND WHY PROVIDER EDUCATION MATTERS
The other major issue we advocated for was clinician education.
Let me say something very directly.
You may sit across from a doctor, nurse practitioner, physician assistant, or specialist and assume they know everything about dementia because they are the medical professional.
And I understand why.
There is authority bias.
You see the white coat. You see the degrees on the wall. You hear the title. You assume, “They know what to do.”
But what if they were trained 20 or 30 years ago?
What if they were trained in a time when we did not have today’s blood-based biomarkers, newer treatment discussions, care navigation models, or the latest dementia-care frameworks?
What if they do not feel confident diagnosing dementia?
What if they do not know how to guide a family through the next step?
That is not an insult to clinicians.
It is reality.
The field has changed.
And medicine has to change with it.
I used this example in the video: some clinicians are practicing like we are still in the Blockbuster era.
But the world has moved to Netflix.
You cannot practice dementia care with outdated tools and expect families to get modern support.
Provider education matters because families depend on clinicians to recognize the disease, diagnose it accurately, explain next steps, connect them with support, and understand the treatment and care options that exist today.
If clinicians are not trained, families lose time.
And in dementia care, lost time can be devastating.
THE CAREGIVER IS TOO OFTEN LEFT ALONE
One of the reasons this issue matters so much to me is personal.
Both of my grandmothers had Alzheimer’s disease.
Both of my parents are caregivers.
I see how difficult this disease is inside real families.
I see the exhaustion. The confusion. The guilt. The stress. The 10 PM phone calls. The medication refusal. The bathing refusal. The wandering risk. The behavior changes. The questions nobody prepared the family to answer.
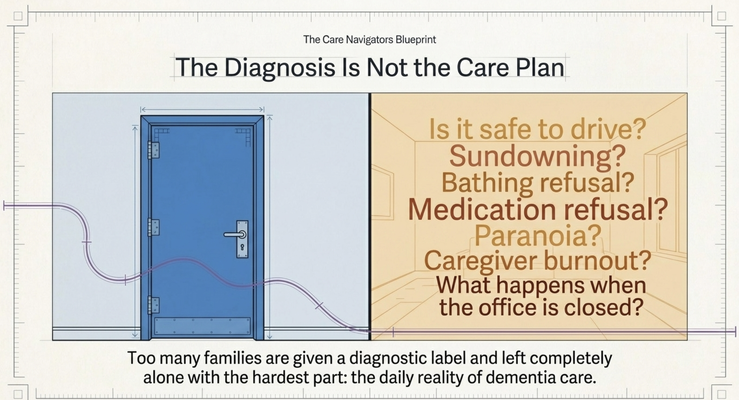
And too often, families are told what the diagnosis is, but not what to do with it.
They are told:
“Your loved one has dementia.”
And then what?
What happens when mom does not want to shower?
What happens when dad refuses medication?
What happens when your loved one gets more confused at night?
What happens when the caregiver is exhausted?
What happens when the person is unsafe at home?
What happens when siblings disagree?
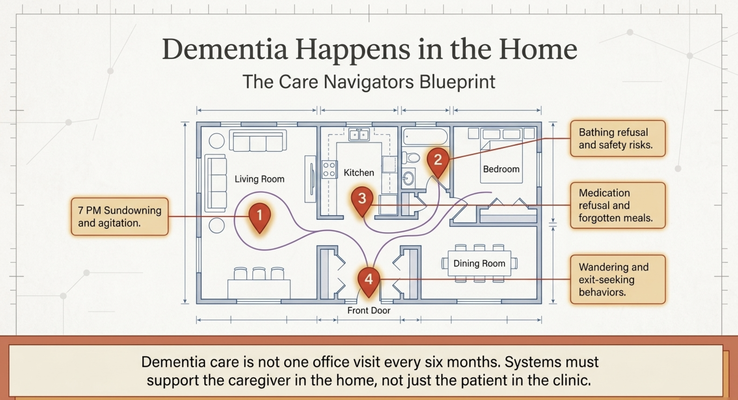
What happens when the doctor visit is over, but the dementia is still happening in the kitchen, the bedroom, the bathroom, and the living room every single day?
This is why advocacy matters.
Because policy cannot only focus on diagnosis.
It has to focus on the caregiving reality after diagnosis.
WHY THE GUIDE MODEL MATTERS
This is exactly why I have dedicated so much of my work to the GUIDE Model.
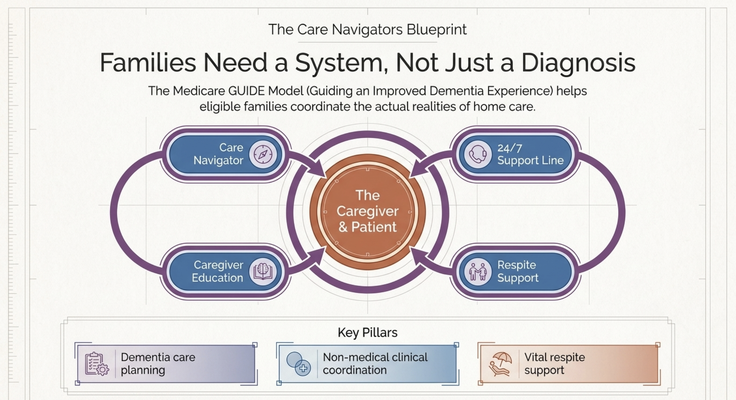
The GUIDE Model — Guiding an Improved Dementia Experience — is a new Medicare model designed to support people living with dementia and the family caregivers caring for them at home.
Through the GUIDE Model, eligible beneficiaries and caregivers may receive structured dementia-care support through organizations like MedBetter Health.
That support may include:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
And I want you to understand why this is so important.
This is not theoretical.
This is what families actually need.
If mom refuses to shower, the caregiver needs someone to call.
If dad refuses medication, the caregiver needs guidance.
If sundowning starts at night, the caregiver needs help.
If the caregiver is exhausted, the caregiver needs respite.
If the family does not know what stage they are in, what questions to ask, or what to prepare for next, they need navigation.
That is what dementia care should look like.
Not a diagnosis and a goodbye.
A system.
A team.
A lifeline.
WHAT I WANT CAREGIVERS TO TAKE FROM THIS
If you are a caregiver reading this, I want you to hear me clearly:
You are not alone.
There are people fighting for you in Washington.
There are advocates telling your story.
There are families standing up and saying, “This disease needs more attention, more funding, more screening, more education, and more support.”
And there are clinicians and care teams working to build better dementia care inside the home.
But I also want you to take action.
If you are noticing memory changes in yourself or someone you love, do not ignore it.
Start the conversation early.
Talk to your doctor.
Ask what testing is appropriate.
Ask whether reversible causes have been ruled out.
Ask about cognitive testing.
Ask about functional changes.
Ask whether a specialist should be involved.
Ask what support exists for the caregiver.
Do not wait until the disease is already causing crisis after crisis.
Early detection is not about fear.
It is about control.
It is about giving families more time, more choices, and a better chance to plan.

THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about Alzheimer’s advocacy, early detection, caregiver support, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Alzheimer’s testing, diagnosis, treatment options, lifestyle interventions, and care planning should be discussed with a qualified healthcare professional.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health