FIRST, UNDERSTAND THE TWO PATHS
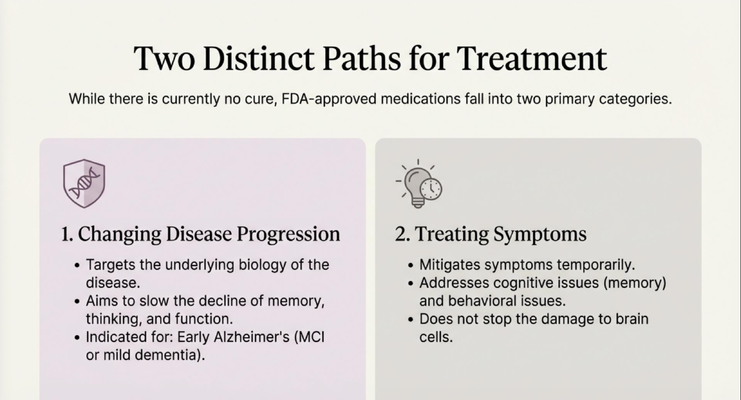
Before I get into the new drugs, I want you to understand something foundational. When it comes to Alzheimer's treatment, there are two completely different categories of medication — and most caregivers do not know the difference.
The first category is medications that treat symptoms. These are the drugs most people are familiar with — they help with memory and cognition temporarily, they address behavioral issues, but they do not stop damage to brain cells. They help bridge the gap. They are not changing the course of the disease.
The second category is medications that change disease progression. These are newer. They target the underlying biology of Alzheimer's — specifically the amyloid plaques building up in the brain — and the goal is to slow how fast the disease advances. This is a fundamentally different approach. And it is what I want to focus on today.
THE PARADIGM SHIFT: A NEW PHASE OF TREATMENT
For a long time, we had no medications that went after the actual cause of Alzheimer's. Everything we had was symptomatic. We were managing the disease, not changing it.
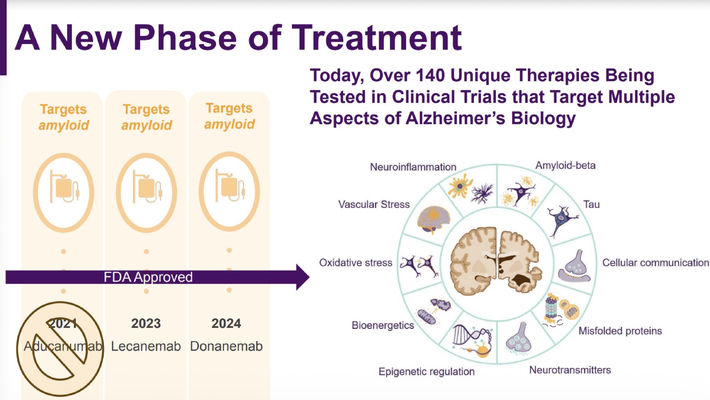
That changed. There are currently over 140 new therapies being studied in clinical trials — targeting amyloid, tau, neuroinflammation, and other aspects of Alzheimer's biology. But two of those drugs have already made it through — they are FDA-approved and available right now.
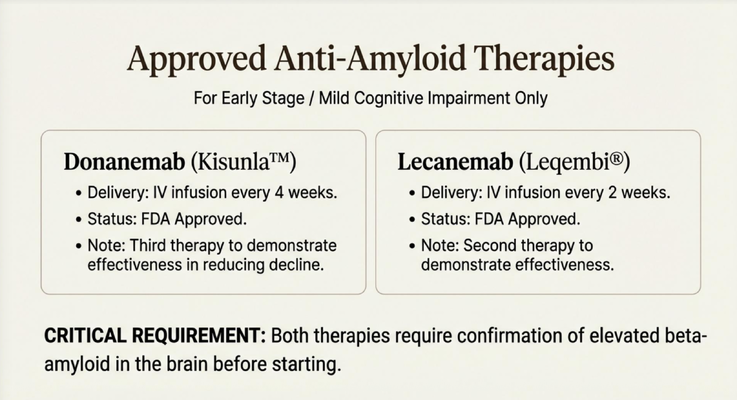
In 2023, lecanemab (brand name Leqembi) was approved. In 2024, donanemab (brand name Kisunla) followed. Both of these are what we call anti-amyloid monoclonal antibodies. That sounds complicated. Let me explain what it actually means.
WHAT ARE THESE DRUGS AND HOW DO THEY WORK?
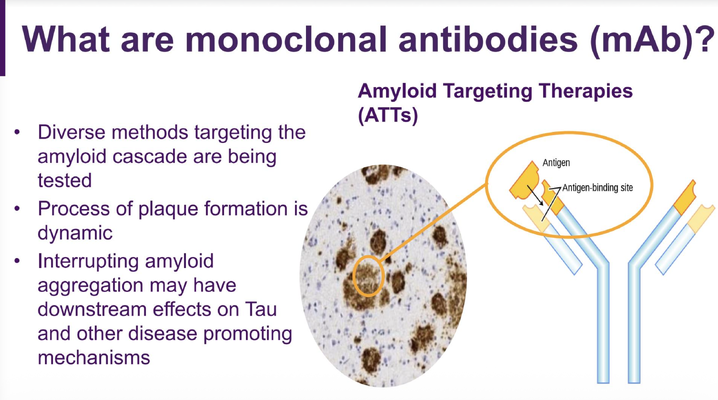
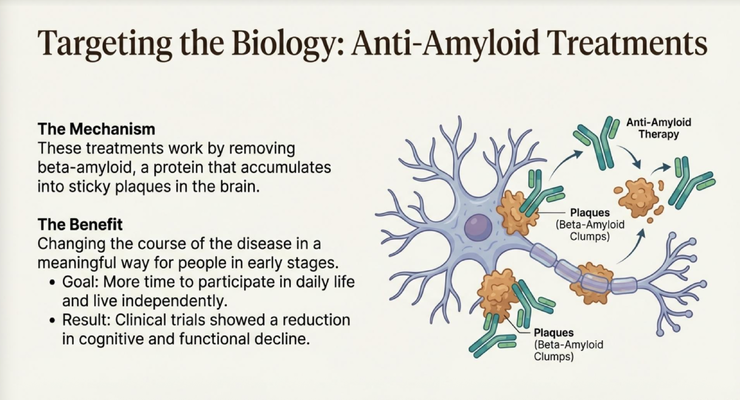
Think of it this way. In a brain affected by Alzheimer's, sticky plaques made of a protein called beta-amyloid build up and accumulate — inside the brain tissue and inside the blood vessels. These plaques are thought to be one of the primary drivers of memory loss and cognitive decline.
What these new drugs do is essentially send your immune system after those plaques. The monoclonal antibodies bind to the amyloid and help clear it out of the brain. Remove the plaques — and the theory, supported by clinical data, is that you slow the progression of the disease.
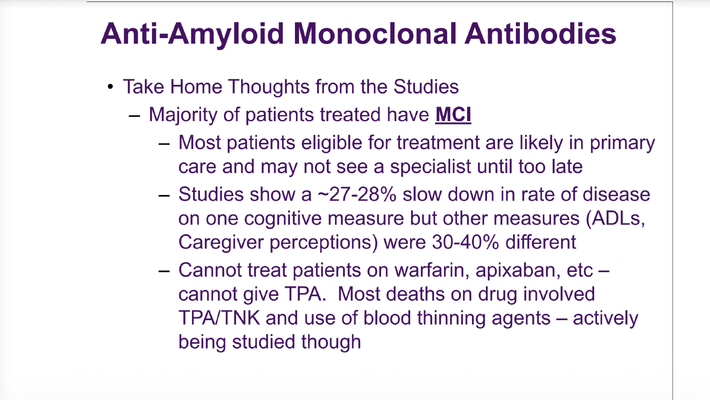
The studies show approximately a 27 to 30 percent slowdown in the rate of cognitive decline. That is not a cure. Your loved one is not going to get their memory back. But slowing the progression of Alzheimer's by 30 percent — buying more time, preserving function longer, maintaining independence for longer — that is significant. That is a number worth having a conversation with your neurologist about.
WHO IS IT FOR AND HOW DO YOU GET IT?
This is the most important thing I want you to take away from this issue: these medications are only for people in the earliest stages. They are indicated for mild cognitive impairment — what we call MCI, which is pre-dementia — and for early-stage mild dementia. If your loved one has moderate or severe dementia, these drugs are not going to be beneficial for them and will not be indicated.
That means the window matters. A lot. Most patients who are eligible are currently being seen by primary care physicians and may not see a neurologist until it is too late. If you are noticing early memory changes in yourself or a loved one, do not wait. See a neurologist now — not in six months.
Both medications are administered as IV infusions — not a pill, not a patch. You go to a specialized clinic, they access an IV, and you receive the medication directly into the bloodstream. Lecanemab is administered every two weeks. Donanemab is administered every four weeks. Both are FDA-approved. Before starting, your neurologist needs to confirm that amyloid is actually present in the brain — through imaging or other non-invasive testing. There is no point removing amyloid that is not there.
THE SIDE EFFECT YOU NEED TO KNOW ABOUT: ARIA
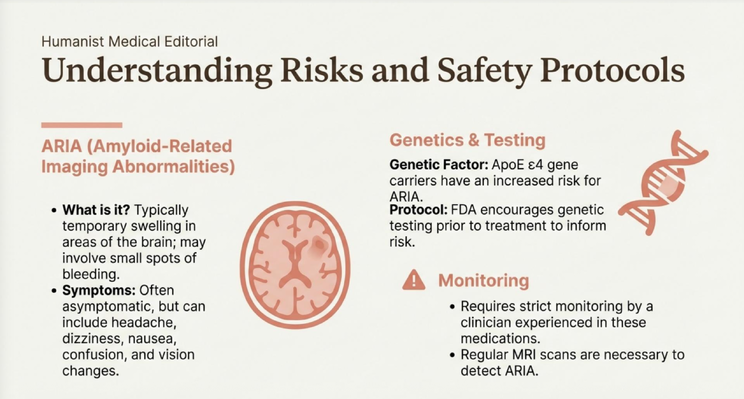
I am not going to tell you only the good news. These drugs come with a side effect called ARIA — Amyloid-Related Imaging Abnormalities. Here is what that means in plain language.
When the drug starts breaking down the amyloid plaques inside the blood vessels, those vessels can become temporarily weaker. What we see in some patients is either a small amount of swelling in the brain — edema — or in some cases a small amount of bleeding — hemorrhage. Many people are completely asymptomatic and never feel a thing. Others may experience headache, dizziness, nausea, or confusion. It depends on how significant the changes are.
There is also a genetic factor. Patients who carry a specific gene variant called APoE ε4 have a higher risk of ARIA. The FDA recommends genetic testing before starting treatment so that you can have an informed conversation about your specific risk level. And while on these medications, regular MRI scans are required to monitor for any of these changes and catch them early if they appear.
I am not telling you this to scare you away from these medications. I am telling you so that you go into the conversation with your neurologist prepared. Because this medication does work — and the risks need to be weighed honestly against the potential benefit of slowing the disease.
WHAT YOU NEED TO DO
The takeaway is simple. The majority of patients who have been treated with these new drugs had mild cognitive impairment — not full-blown dementia. That means if your loved one is in the early stages of memory decline, the window to access these treatments is now. Not later. Now.
See a neurologist. Have the amyloid confirmed. Discuss APOE genetic testing. Understand the monitoring requirements — regular MRIs, regular infusions, commitment from both the patient and the caregiver. And make a decision based on the real risks and real benefits for your specific situation.
Do not wait until the disease has progressed past the point where these options are available.
The Invisible Weight: Caregiver Exhaustion
Navigating a dementia diagnosis is overwhelming under any circumstances. Now layer on top of that trying to understand a rapidly evolving treatment landscape — new drugs, new clinical trials, genetic testing, specialist referrals — while also managing the day-to-day reality of caregiving.
Most families are doing all of this alone. With no guidance, no navigator, and no one who can sit with them and walk them through what it all means.
You should not have to do this alone. And thanks to a new Medicare program, you don't have to.
The GUIDE Model: Medicare's New Dementia Care Program
MedBetter Health is proud to participate in Medicare's GUIDE Model — Guiding an Improved Dementia Experience. This 8-year CMS initiative is transforming dementia care nationwide.
Through the program, eligible beneficiaries and their caregivers receive:
- A dedicated Care Navigator who is available during business hours and coordinates all aspects of care
- A 24/7 helpline for non-medical behavioral emergencies — for when you don't know what to do at 2am
- Medicare-covered respite care so you can take a real break while someone qualified stays with your loved one
- Caregiver education, training, and personalized dementia care plans
To be eligible, your loved one needs a clinician-confirmed dementia diagnosis and Medicare Parts A and B. Medicare Advantage plans do not qualify. An assessment is required to confirm eligibility.
👉 Check your eligibility for the GUIDE Model Program in under two minutes: https://medbetterhealth.org/guide
📍 MedBetter Health currently serves families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting every caregiver with practical, evidence-based education.
Straight Talk With Dr. Erik

Learn more about new Alzheimer's treatments. Watch the full video and subscribe for regular insights.
https://www.youtube.com/@ErikIlyayev
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health