MEDICATION REFUSAL IS MORE COMMON THAN PEOPLE THINK
Let’s start with the numbers.
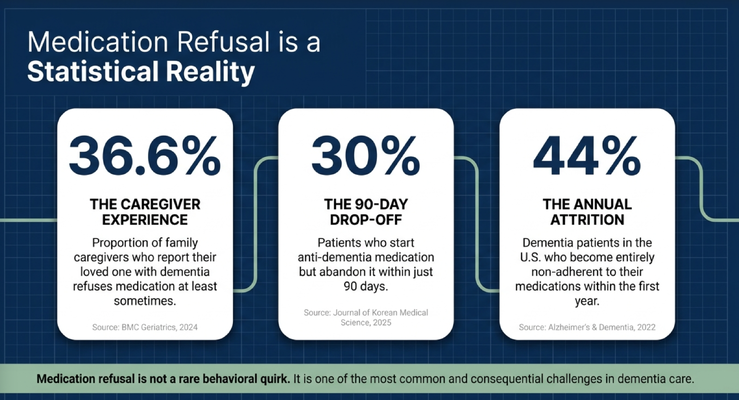
The presentation highlighted that 36.6% of family caregivers report that their loved one with dementia refuses medication at least sometimes. It also showed that 30% of patients who start an anti-dementia medication abandon it within 90 days, and 44% of dementia patients in the United States become entirely non-adherent to their medications within the first year.
That means medication refusal is not a strange exception.
It is a statistical reality.
And if you are a caregiver dealing with this, you already know the emotional side of it. It does not feel like a statistic when it is happening at your kitchen table.
It feels like pressure.
You may be thinking, “If she does not take this, what happens?” You may be worried about blood pressure, diabetes, memory medication, heart medication, mood medication, or a medication the doctor specifically told you was important. You may feel guilty because you cannot get your loved one to cooperate. You may feel angry because you are trying to help and they are accusing you of hurting them.
This is why medication refusal needs a framework.
Because without a framework, the caregiver often ends up in a daily argument.
THE COST OF NON-ADHERENCE IS NOT ONLY FINANCIAL
When a loved one refuses medication, the impact can build quickly.
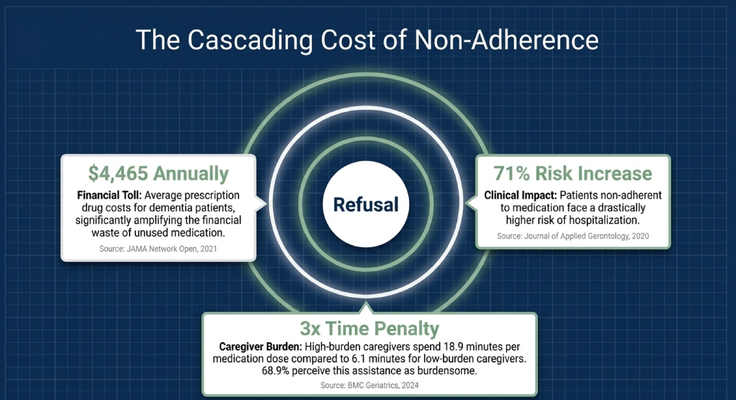
The presentation highlighted an average annual prescription drug cost of $4,465 for dementia patients, which becomes especially frustrating when medications are filled, brought home, and then left unused in a cabinet.
I saw this all the time when I used to do house calls.
I would walk into someone’s home, open a closet to hang my coat, and there would be bags and bags of unused medication. Bottles sitting there. Pills that were prescribed, filled, paid for, and never taken.
But the larger issue is not only financial waste.
The larger issue is clinical risk.
The presentation highlighted that patients who are non-adherent to medication face a significantly higher risk of hospitalization. Now, I want to be very clear: I am not saying every medication is always right forever. Medications should be reviewed. You should ask questions. You should understand why a medication was prescribed, who prescribed it, what the side effects are, and whether it still makes sense.
But once you and the medical team have determined that a medication is necessary, refusal becomes a serious care issue.
It can increase caregiver stress. It can worsen medical instability. It can lead to avoidable crises. And it can turn the caregiver’s role into a daily battle of persuasion, pressure, and guilt.
That is not sustainable.
REFUSAL IS NOT THE DIAGNOSIS. IT IS THE SYMPTOM.
Here is the most important shift.
Medication refusal is not the diagnosis.
It is the symptom.
When a person living with dementia refuses medication, the first instinct is often to label the behavior:
“She is stubborn.”
“He is difficult.”
“She just does not listen.”
“He is being impossible.”
But that usually does not help.
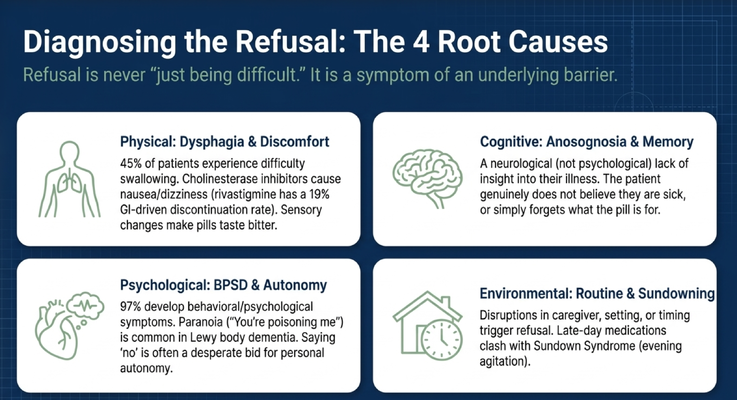
The better question is: what is the barrier underneath the refusal?
There are four major categories I want caregivers to think about.
The first is physical. Your loved one may have dysphagia, which means difficulty swallowing. This is very common in dementia. If swallowing is difficult or frightening, then a pill is not just a pill. It is a threat. Some medications can also cause nausea, dizziness, stomach discomfort, or other side effects that make the person associate pills with feeling worse.
The second is cognitive. A person living with dementia may not believe they are sick. They may not understand why they need medication. They may truly believe nothing is wrong. So when you say, “You need to take this,” their brain may interpret that as unnecessary, confusing, or intrusive.
The third is psychological. Dementia can create paranoia, suspicion, fear, or altered reality. A loved one may believe the medication is poison. They may believe the caregiver is trying to control them. They may think, “You are giving this to me because you want my money,” or, “You are trying to hurt me.”
That sounds irrational to us, but to the person living with dementia, the fear can feel completely real.
The fourth is environmental. Maybe the medication is being offered at the wrong time of day. Maybe it is during sundowning. Maybe a new caregiver is offering it. Maybe the room is loud. Maybe the routine changed. Maybe the person is tired, overstimulated, or already upset before the pill ever appears.
So before we force, argue, or repeat ourselves, we have to ask:
Is this physical?
Is this cognitive?
Is this psychological?
Is this environmental?
Because if you do not know the reason, you may use the wrong solution.
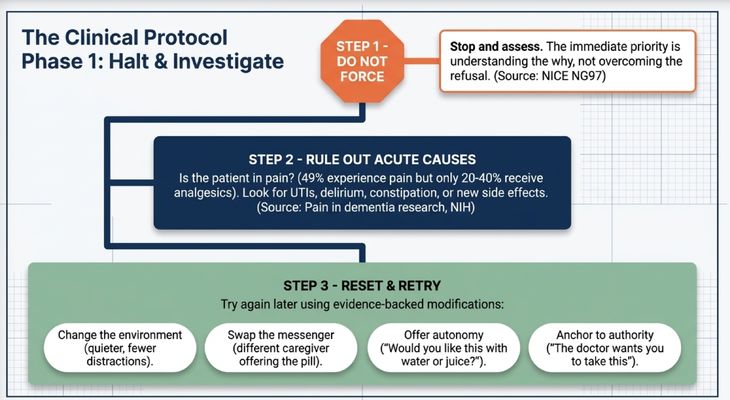
STEP ONE: DO NOT FORCE
This is where caregivers need to pause.
If your loved one refuses medication, the first step is not to overpower them.
The first step is to stop and assess.
I am not saying the medication does not matter. I am not saying to ignore important prescriptions. I am not saying to make medical decisions on your own.
I am saying that in that specific moment, when the person is refusing and emotionally activated, forcing often makes the problem worse.
Why?
Because now the medication becomes associated with fear, pressure, and loss of control. The next time the caregiver approaches with the pill cup, the person remembers the emotion even if they do not remember the exact event.
They may not say, “Yesterday you pressured me and I felt scared.”
But the body remembers the threat.
So step one is simple:
Do not force.
Pause. Step back. Ask what might be happening. Look at the environment. Look at the timing. Look at the person’s face and body language. Are they afraid? Are they angry? Are they confused? Are they uncomfortable? Are they in pain?
The immediate goal is not to win the battle.
The immediate goal is to understand the refusal.
STEP TWO: RULE OUT ACUTE CAUSES
The second step is to rule out acute causes.
Was there a sudden change?
Did they take medication normally before and now they refuse? Is there a new caregiver? A new medication? A new dose? A new setting? A urinary tract infection? New confusion? New pain? New constipation? Poor sleep? A recent hospitalization? A change in routine?
Sudden behavior changes in dementia should always make us ask medical questions.
Sometimes the refusal is not about the pill itself. It may be that the person feels sick, scared, uncomfortable, or disoriented and cannot explain it clearly.
For family caregivers, this means you should not assume, “This is just dementia.”
For professional caregivers and home care agencies, this means medication refusal should be documented and communicated. If the pattern changes suddenly, the family and clinical team need to know.
The person living with dementia may not be able to advocate for themselves clearly.
So the behavior becomes the message.
STEP THREE: RESET AND RETRY
Once you pause and assess, the next step is often to reset and retry later using a different approach.
There are several practical adjustments that may help.
First, change the environment. If medication is always offered in the same chair, same room, or same tense moment, the person may associate that setting with a negative experience. Try changing the location. Move to a calmer room. Reduce noise. Remove distractions. Try again when the person is more relaxed.
Second, swap the messenger. Sometimes one caregiver has become associated with the medication battle. A different family member, aide, nurse, or trusted person may get a different response. This does not mean the first caregiver failed. It means dementia is emotional. The messenger matters.
I saw this with my own grandmother. Sometimes my aunts had trouble getting her to take medication, and then I would come in and say, “Come on, Grandma, I’d really love for you to take this,” and she would take it. Same medication. Different messenger. Different emotion.
Third, offer autonomy.
This is a big one.
A person living with dementia is losing control over so many parts of life. When we approach medication like an order, it can feel like one more thing being taken away.
So instead of saying, “Take this now,” try offering choices.
“Would you like to take the blue pill first or the white pill first?”
“Would you like water or juice?”
“Would you like to take it now or in five minutes?”
The key is that the medication still matters, but the person gets some sense of control in the process.
Fourth, anchor to authority.
Some people living with dementia still respond to a trusted physician, pharmacist, or clinician. You might say, “Dr. Wiley wanted you to take this today,” or show a written note from the doctor if that helps. The point is not to scare the person. The point is to connect the action to someone they trust.
Again, the goal is not force.
The goal is cooperation.
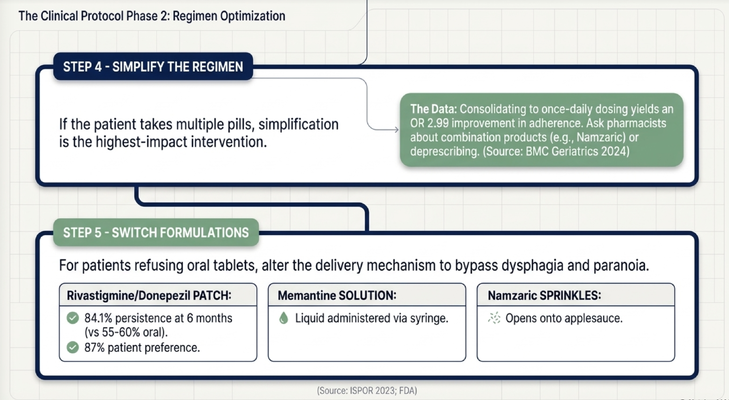
SIMPLIFY THE REGIMEN BEFORE YOU STRUGGLE
There is another major step caregivers often miss.
Simplify the regimen.
Now, this must be done with the prescribing clinician and pharmacist. Do not stop, combine, crush, split, open, or change medications on your own without professional guidance.
But you can ask better questions.
If your loved one takes six medications three times a day, that is a lot. It may have happened slowly over years. One doctor adds one medication. Another doctor adds another. A hospital discharge adds something else. Before you know it, the caregiver is managing a complicated schedule that would overwhelm almost anyone.
So ask the doctor or pharmacist:
Can any medications be discontinued safely?
Can the schedule be simplified?
Can anything be changed from three times a day to twice a day or once a day?
Are there combination medications?
Are there medications that are no longer necessary?
Are there side effects that may be making adherence harder?
Sometimes simplification is the highest-impact intervention.
Not because the caregiver tried harder, but because the system became easier.
SWITCHING FORMULATIONS MAY HELP
Another practical option is changing the formulation.
Some people have trouble swallowing tablets. Others become suspicious when they see pills. Others experience stomach discomfort or refuse because the pill is too large, bitter, or difficult.
Depending on the medication, there may be alternatives. Some medications may have patch options. Some may have liquid formulations. Some may have sprinkle capsules or other delivery methods.
But again, this has to be done through the prescriber or pharmacist.
Do not assume a medication can be crushed, mixed into food, opened, or changed. Some medications are dangerous to alter because of how they are absorbed or released in the body.
The caregiver’s job is not to experiment blindly.
The caregiver’s job is to ask the right questions and bring the care team into the problem.
Because sometimes the issue is not that your loved one “will not cooperate.”
Sometimes the regimen is too complicated.
Sometimes the pill is too hard to swallow.
Sometimes the timing is wrong.
Sometimes the formulation is wrong.
Sometimes the side effects are the reason the person is resisting.
And sometimes the solution starts with a phone call to the doctor or pharmacist.
WHAT CAREGIVERS SHOULD REMEMBER
If medication refusal is happening in your home, here is what I want you to remember.
Do not start with force.
Start with why.
Is there pain? Is there swallowing difficulty? Is there paranoia? Is there confusion? Is there a new caregiver? Is the timing wrong? Is sundowning involved? Is the medication causing side effects? Is the person trying to preserve control?
Once you understand the why, the solution becomes more targeted.
Maybe the answer is changing the environment.
Maybe it is trying again later.
Maybe it is using a different caregiver.
Maybe it is offering choices.
Maybe it is asking the physician to simplify the regimen.
Maybe it is asking the pharmacist about an alternative formulation.
Maybe it is evaluating for an acute medical issue.
But if you skip the “why,” you are guessing.
And in dementia care, guessing creates frustration for everyone.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly the type of issue caregivers should not have to navigate alone.
Medication refusal is not just a pill problem. It is a dementia care problem. It involves communication, routine, medical review, caregiver stress, environmental triggers, swallowing concerns, cognition, trust, and safety.
That is why Medicare created the GUIDE Model — Guiding an Improved Dementia Experience.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because caregivers need more than a list of instructions.
They need someone who can help them think through real situations:
What do I do if mom refuses her medication?
How do I know if this is pain, fear, paranoia, or swallowing difficulty?
When should I call the doctor?
How do I talk to the pharmacist?
How do I reduce the argument and keep the person safe?
That is the type of guidance caregivers need inside the home.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about medication refusal, caregiver strategies, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Do not start, stop, crush, split, hide, mix, or change any medication without guidance from the prescribing clinician or pharmacist. If medication refusal begins suddenly or is associated with new confusion, pain, weakness, fever, falls, aggression, or other concerning symptoms, contact a qualified healthcare professional promptly.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health