THE SCALE OF THE PROBLEM
Before we talk about behaviors, we have to talk about the scale of dementia care.
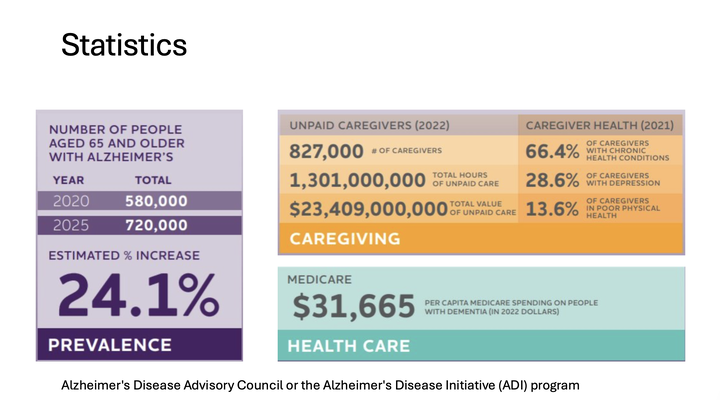
In Florida alone, the number of people age 65 and older living with Alzheimer’s disease has been rising sharply. The presentation highlighted a projected increase from 580,000 people in 2020 to 720,000 people in 2025.
That is a 24.1% increase.
But numbers like that are not just statistics. They represent families. They represent spouses who are now caregivers. Adult children who are trying to keep mom or dad safe. Home care agencies trying to support complicated cases. Nurses, physicians, social workers, and community organizations trying to respond to a growing need.
And behind every person living with dementia, there is often an unpaid caregiver trying to hold the entire system together.
That caregiver may be managing medications, meals, appointments, bathing, nighttime confusion, wandering risk, family conflict, finances, transportation, and their own job at the same time.
So when we talk about behavioral symptoms in dementia, we are not talking about an isolated medical issue.
We are talking about what happens inside the home, every day, when the disease meets real family life.
BEHAVIOR IS COMMUNICATION
One of the most important ideas in dementia care is this:
Behavior is communication.
When a person living with dementia becomes angry, agitated, fearful, suspicious, restless, or resistant, the behavior is usually not the whole story. The behavior is the visible part. The deeper question is: what is underneath it?
What happened right before the behavior?
Was the room too loud? Was the person tired? Was there a change in routine? Was the caregiver rushing? Was the person in pain? Was there a urinary tract infection? Was the room too dark? Did a shadow look like a person? Did the person feel trapped? Did they misunderstand where they were?
This is where I want families to think less like judges and more like detectives.
A judge looks at the behavior and says, “That was wrong.”
A detective asks, “What caused this?”
In dementia care, that question changes everything.
If mom is yelling, we ask what she is feeling. If dad is pacing, we ask what need is not being met. If grandma is refusing the shower, we ask what part of the shower experience feels threatening. If a loved one is trying to leave the house, we ask what they believe they need to do.
For home care agencies and care teams, this is where training matters. The aide walking into the home needs more than a task list. They need to understand how to observe patterns, report changes, and respond calmly when the behavior escalates.
The behavior is not the starting point and the ending point.
It is a clue.
ALTERED REALITY: WHEN THE BRAIN MISREADS THE WORLD
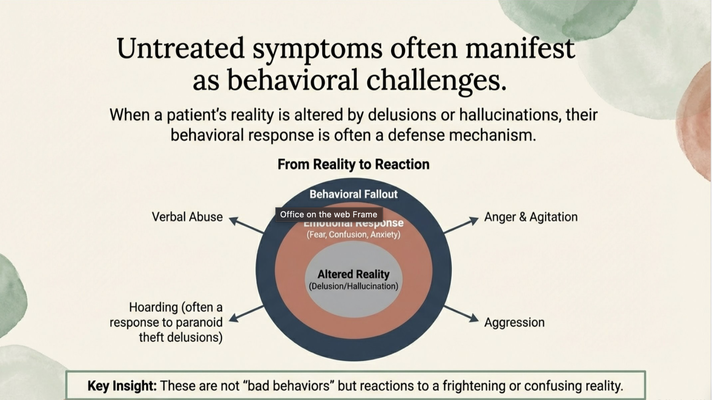
A lot of behavioral symptoms come from altered reality.
A delusion is a false belief the person accepts as absolute truth. A common example is the “stolen item” delusion. The person misplaces a purse, forgets where it is, and then believes someone stole it. Another common example is believing a spouse is being unfaithful because the person cannot account for where the spouse was during part of the day.
A hallucination is different. A hallucination is a sensory experience. The person may see, hear, or feel something that is not physically present.
To the caregiver, it may seem obvious.
“No one stole your purse.”
“There is no one in the room.”
“You are already home.”
“Your spouse was just at the store.”
But to the person living with dementia, it feels real.
That is the part families have to understand. If the person believes someone stole their purse, they are not pretending. If they see someone standing in the hallway, they are not trying to be difficult. If they believe they need to go home, even though they are already home, they are not just being stubborn.
Their reality has been altered by dementia.
And when you respond with logic, you may accidentally increase fear.
This is where families often get stuck. They say, “Dr. Erik, why is my mom being so mean?” Or, “Why is dad suddenly aggressive?” Or, “Why does she keep accusing me of things I would never do?”
And I always try to reframe it.
The person may not be trying to hurt you. The person may be trying to defend themselves from a reality that feels frightening.
If someone truly believes their purse was stolen, anger makes sense. If someone truly believes a stranger is in the room, fear makes sense. If someone truly believes you are preventing them from going home, resistance makes sense.
That does not mean the behavior is easy. It does not mean caregivers should tolerate unsafe situations. It does not mean we ignore aggression or safety risk.
But it does change how we respond.
We stop asking, “How do I prove them wrong?”
And we start asking, “What are they experiencing, and how do I lower the distress?”
Because many behaviors are not “bad behaviors.” They are reactions to a frightening or confusing reality.
DO NOT JUMP STRAIGHT TO “IT’S THE DEMENTIA”
Another major point from the presentation was this:
Do not blame every sudden behavior change on dementia.
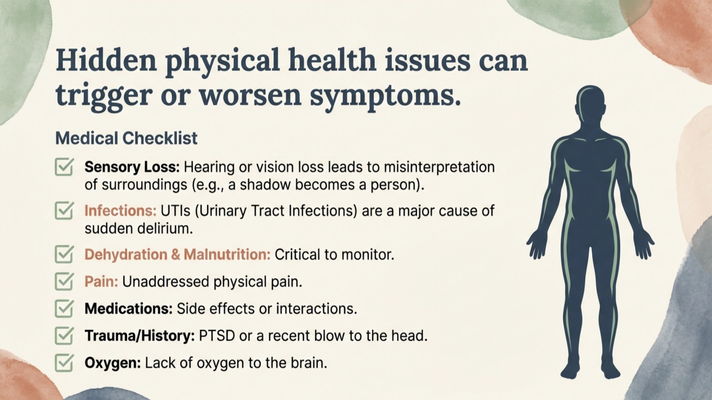
Dementia may be the background condition, but sudden worsening can be caused by something else.
Hearing loss can cause misinterpretation. Vision loss can make shadows look like people. A urinary tract infection can trigger sudden confusion or delirium. Dehydration, malnutrition, constipation, pain, medication changes, medication side effects, trauma, poor sleep, or low oxygen can all worsen behavior.
This matters because the person living with dementia may not be able to explain what is wrong.
They may not say, “I have pain.”
They may not say, “I feel burning when I urinate.”
They may not say, “I cannot see well in this room.”
They may not say, “This medication is making me feel strange.”
Instead, the body speaks through behavior.
So if a behavior changes suddenly, especially over hours or days, that is a red flag. Families should speak with a qualified healthcare professional and look for medical causes, not just assume the dementia got worse overnight.
For professional caregivers, this is one of the most important points. A sudden change in behavior should not be treated as “just dementia.” It should be documented, communicated, and evaluated. The caregiver in the home may be the first person to notice the change.
Behavioral symptoms deserve assessment, not dismissal.
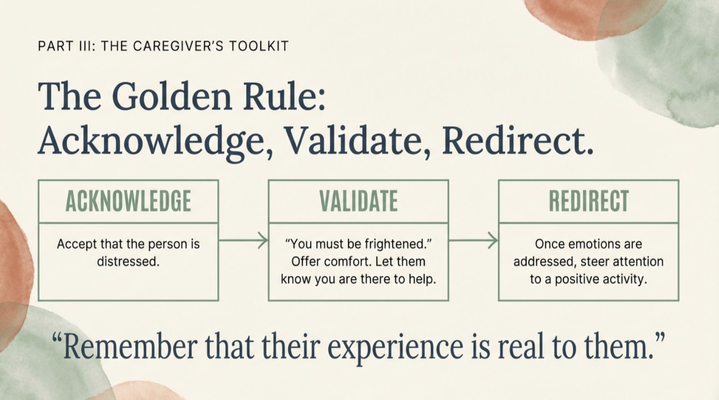
THE CAREGIVER’S FIRST RESPONSE: ACKNOWLEDGE, VALIDATE, REDIRECT
When a person living with dementia is distressed, the caregiver’s instinct is often to correct.
“That is not true.”
“No one stole your purse.”
“You already live here.”
“Your mother passed away years ago.”
“You cannot go home.”
But logic is often ineffective once the person is emotionally activated.
The better framework is:
Acknowledge. Validate. Redirect.
Acknowledge means you accept that the person is distressed. You do not have to agree with the false belief, but you do have to recognize the emotion.
Validate means you respond to the feeling underneath the statement.
Redirect means once the emotion is addressed, you gently move attention toward something safer, calmer, or more familiar.
So if someone says, “I need to go home,” the worst response is often, “You can’t go home. You live here now.”
That may be factually true, but emotionally it can feel like a prison sentence.
A better response might be:
“I can see you’re worried about your house. You’re safe here with me. Tell me about your garden.”
Now we are not fighting the belief. We are meeting the emotion.
That is the difference between correction and care.
I know this is hard, especially when the accusation feels personal. When someone you love accuses you of stealing, lying, abandoning them, or keeping them trapped, it hurts. Especially when you are the one showing up every day.
But in dementia care, their reality has often been altered. They are not always responding to you as you are. They are responding to the reality their brain is creating in that moment.
That is why connection is more effective than correction.
Remain calm. Avoid arguments. Be supportive. Lower the emotional temperature before trying to solve the problem.
If you can de-escalate the emotion, you often reduce the behavior.
And if you keep trying to prove the person wrong, you may win the fact and lose the trust.
Trust matters. Once trust breaks in that moment, everything else becomes harder. Bathing becomes harder. Eating becomes harder. Medication becomes harder. Redirecting becomes harder. The entire day can spiral.
So do not make logic your first tool.
Make connection your first tool.
SUNDOWNING: WHEN THE DAY BECOMES TOO MUCH
Another behavior families ask about constantly is sundowning.
Sundowning is not random. It often happens when multiple pressures collide at the end of the day: fatigue, sensory overload, changing light, disrupted circadian rhythm, hunger, dehydration, pain, boredom, and the accumulated effort of trying to process the world all day.
By late afternoon, the cognitive battery is lower.
The person may begin pacing, shadowing the caregiver, asking to go home, becoming anxious, or becoming more suspicious.
This does not always mean something terrible happened in that moment. It may mean the brain has reached its limit.
That is why the evening routine matters.
Close blinds before reflections become frightening. Turn on warm lighting before shadows build. Reduce stimulation. Avoid loud television or distressing news. Keep the sequence predictable. Offer food, fluids, toileting, comfort, and familiar activities before the person becomes overwhelmed.
The goal is not to overpower sundowning once it starts.
The goal is to lower the triggers before the brain enters crisis mode.
WANDERING: RISK, NEED, AND DIGNITY
Wandering is one of the most frightening dementia behaviors for families.
And for good reason.
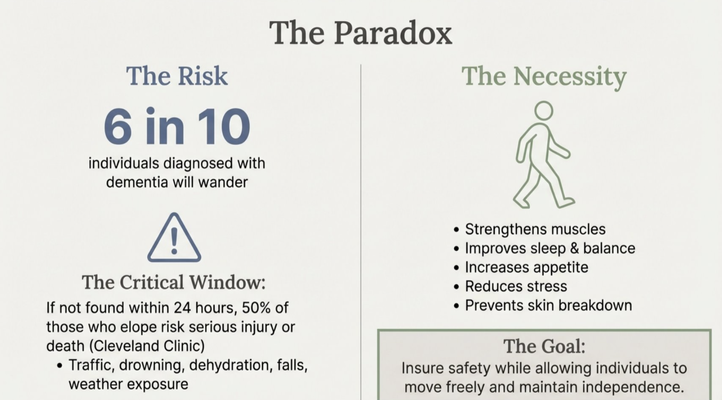
The presentation highlighted that 6 in 10 individuals diagnosed with dementia will wander. It also emphasized that if someone who elopes is not found within 24 hours, the risk of serious injury or death becomes extremely high.
So yes, wandering is a safety issue.
But here is the nuance: movement itself is not the enemy.
Walking can strengthen muscles, improve balance, increase appetite, reduce stress, support sleep, and preserve independence. The goal is not to lock the person into immobility. The goal is to allow safe movement while preventing dangerous elopement.
That is the paradox of wandering.
We have to protect the person without stripping away every bit of freedom.
A major mistake in dementia care is treating all wandering as the same behavior.
It is not.
There is goal-oriented walking. The person is moving with purpose, maybe looking for the bathroom, trying to help, or repeating an old routine.
There is pacing. This can be repetitive movement that signals anxiety, boredom, discomfort, or an unmet need.
There is getting lost. The person may be in a familiar place but can no longer use their internal map.
Then there is critical wandering or elopement, where the person leaves a secure area without safety awareness. That is the highest-risk category.
The intervention depends on the type.
If the person is pacing because they are anxious, the answer may be reassurance and structured activity.
If they are wandering because they need the bathroom, the answer may be scheduled toileting and better signage.
If they are leaving because they believe they need to go to work or pick up children, the answer may be validation, redirection, and meaningful engagement.
Again, behavior is communication.
Wandering is no different.
THE ICEBERG UNDER THE BEHAVIOR
When a person wanders, the walking is only what we see on the surface.
Underneath may be memory loss, disorientation, sundowning, pain, constipation, hunger, thirst, medication side effects, boredom, loneliness, anxiety, fear, or a desire to return to a past role.
A retired teacher may believe they need to go to school.
A former parent of young children may believe they need to pick up the kids.
A person who worked every day for 40 years may believe they are late for a shift.
To the caregiver, it looks like wandering.
To the person, it may feel like responsibility.
That is why meaningful engagement matters. If a person is searching for purpose, simply blocking the door may not solve the distress. But giving them a safe role, a structured activity, a walk, a folding task, music, familiar objects, or a calming routine may reduce the need to leave.
This is where home care teams can make a major difference. The best care is not just watching someone. It is learning who they were, what roles mattered to them, what routines shaped their life, and how to give them safe ways to still feel useful.
The question is not only, “How do I stop the wandering?”
The better question is, “What need is the wandering trying to meet?”
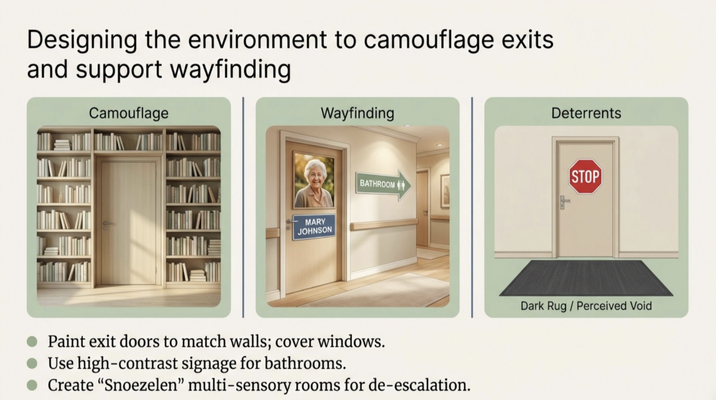
ENVIRONMENTAL DESIGN IS PREVENTION
For wandering risk, the home environment matters.
Camouflaging exit doors, covering door windows, using high-contrast bathroom signs, improving lighting, creating safe walking paths, and reducing exit cues can all help.
A coat by the door may cue leaving. Keys visible on the counter may cue leaving. Someone else walking out the door may cue leaving. A dark hallway may increase fear. A confusing layout may increase disorientation.
In dementia care, prevention often happens before the crisis.
We do not wait until someone is outside and missing to think about the environment. We look at the patterns early.
What time of day does the wandering happen? What happened right before? What does the person seem to be looking for? Are they bored? Are they anxious? Are they trying to complete an old responsibility? Are there environmental cues pushing them toward the door?
Once we know the pattern, we can design around it.
That is the difference between reacting and preventing.
ROUTINE, PURPOSE, AND STRUCTURED ENGAGEMENT
One of the strongest non-medication tools we have in dementia care is routine.
A predictable day reduces anxiety. Meaningful activity reduces restlessness. Scheduled walking reduces the need to wander at unsafe times. Familiar tasks reduce agitation because they give the person something recognizable to do.
And this connects directly to dignity.
I shared a story about my grandmother, who loved washing dishes. To me, washing dishes was just washing dishes. But to her, it was how she helped. It was how she contributed. It was her role.
When I saw water on the floor, my first instinct was safety. Water means fall risk. Fall risk means injury. Injury can mean hospitalization. So the logical response was, “No more dishes.”
But then she became quieter. She stayed in her room more. She was not engaging the same way.
And I realized something important.
I did not just take away the dishes.
I took away her purpose.
That is the kind of mistake families make with the best intentions.
Safety matters. Of course it matters. But before we remove an activity completely, we should ask: can we adapt it?
Can we use a non-slip mat? Can we supervise? Can we let her rinse one plate instead of washing the whole sink? Can we let her fold towels, even if we refold them later? Can we let her set the table?
The goal is not perfection.
The goal is purpose.
Because dementia changes memory. It changes communication. It changes behavior. But it does not erase the human need to matter.
That is why the best dementia care is not only about preventing harm. It is about preserving identity.
FROM RESTRICTION TO SUPPORT
If there is one theme I wanted families and professionals to leave with, it is this:
We have to move from restriction to support.
Restriction alone says, “Stop walking.”
Support asks, “Why are you walking, and how do we make it safe?”
Restriction says, “Stop asking for your mother.”
Support asks, “What feeling is this person expressing, and how do we comfort them?”
Restriction says, “No more dishes.”
Support asks, “How can we preserve the role while lowering the risk?”
Restriction says, “That is not real.”
Support says, “I know this feels real to you, and I am here with you.”
This is the heart of dementia care.
Understand the behavior. Validate the feeling. Secure the safety.
For caregivers, this means you do not have to solve every behavior by force. You can slow down, look for the trigger, meet the emotion, and change the environment.
For home care agencies, this means training teams to see behavior as communication, not defiance.
For healthcare professionals, this means sudden changes deserve investigation, and families need practical guidance they can actually use inside the home.
And for the person living with dementia, this means care that protects more than the body. It protects dignity.
WHERE THE GUIDE MODEL FITS IN
This is also why Medicare created the GUIDE Model — Guiding an Improved Dementia Experience.
Dementia care is not one appointment every six months. It is daily life inside the home. It is what happens at 7 PM when sundowning starts. It is what happens when dad tries to leave the house. It is what happens when mom refuses to shower. It is what happens when a caregiver has not slept and does not know what to do next.
Through the GUIDE Model, eligible beneficiaries and caregivers may receive support such as care navigation, caregiver education, care coordination, help building a dementia care plan, and support when caregiving becomes overwhelming.
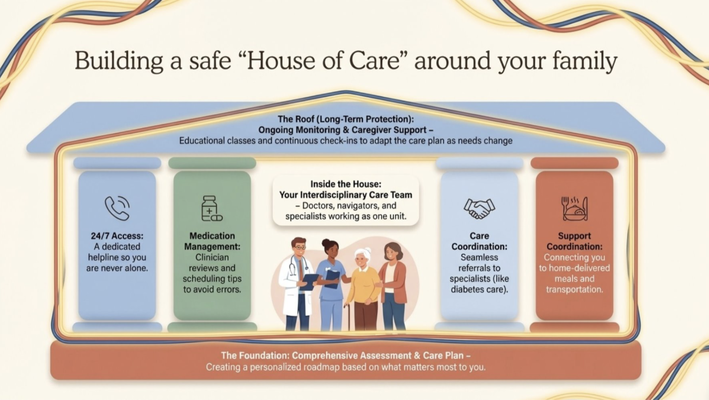
At MedBetter Health, we believe families need more than a diagnosis.
They need a house of care around them.
A care team. A plan. Education. Ongoing support. Help with medication management. Support coordination. A place to call when the next behavioral challenge shows up.
Because dementia care should not be a family guessing alone in the dark.
THE NEXT STEP FOR FAMILIES
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia behaviors, wandering, hallucinations, delusions, sundowning, dignity, and caregiver support by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health