

Alzheimer’s disease, dementia care, and the GUIDE Model.
And I want to start with a story from my own family.
My grandmother is 93 years old. My mother and father are both around 70. My grandmother lives with them, and for many years, I lived in that same home too — my grandmother, my parents, my wife, myself, and my six children all under one roof.
It was a beautiful experience.
A transgenerational experience.
We learned from each other. We lived together. We helped each other.
But I also saw something very real.
My parents are caregivers.
And caregiving is not easy.
One day, I was visiting my grandmother in New York. I walked into the room and heard her ask my mother:
“Where is my mother?”
Now remember, my grandmother is 93. Her mother passed away many years ago.
So my mother did what most people would do.
She used logic.
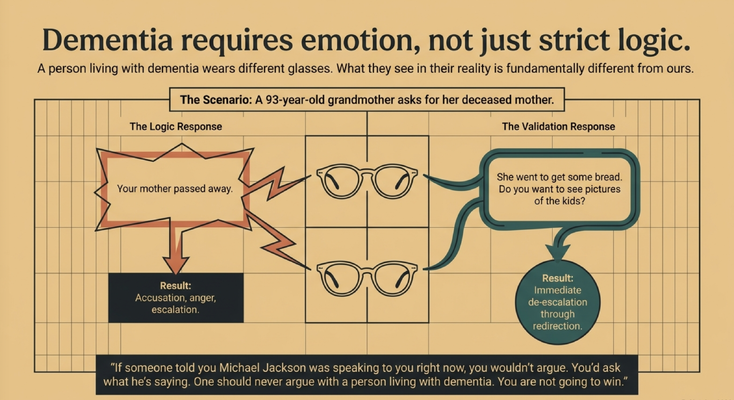
She said, “Mom, your mother passed away.”
And my grandmother looked at her and said something very painful:
“You are the worst daughter-in-law in the world. I regret that I allowed my son to marry you.”
Now, understand this.
My mother has been caring for my grandmother for decades. She is not just a daughter-in-law. She is a daughter to her.
So of course my mother became upset.
And this is where dementia care becomes very different from ordinary caregiving.
Because with dementia, logic does not always solve the problem.
Sometimes logic escalates the problem.
My name is Dr. Erik Ilyayev. I’m a dementia care physician, a board member of the South Florida Alzheimer's Association® , and the CEO of MedBetterHealth.org — one of the organizations selected by Medicare to participate in a groundbreaking new program designed to change how America cares for people living with dementia.
In this issue, I want to explain why dementia care has to move beyond medication alone, why caregivers need support, and why the GUIDE Model represents a real shift from simply reacting to dementia behaviors to helping families navigate them.
DO NOT ARGUE WITH DEMENTIA REALITY
When my grandmother became upset, I stepped in.
I said:
“Grandma, no, no, no. Your mother went shopping. She went to get some bread. Do you want to see pictures of my kids?”
Then I showed her pictures.
“This is Abraham. This is Tipporah. This is Yosef.”
And just like that, the situation de-escalated.
What did I use?
Validation.
Then redirection.
I did not argue with her reality.
I did not say, “Grandma, you are wrong.”
I did not force her to relive the pain of losing her mother.
I met her emotionally first.
Then I moved her somewhere safer.
This is one of the most important things I want families to understand:
You are not going to win an argument with dementia.
Why?
Because the person living with dementia is seeing the world through different glasses.
What they see, what they believe, what they feel in that moment may be completely different from what you and I see.
If someone told you Michael Jackson was speaking to you right now, you would say, “What are you talking about? That is not Michael Jackson.”
Now imagine someone kept arguing with you.
That is what dementia can feel like.
The person’s reality is not matching ours. And if we keep trying to force them into our reality, we may create fear, anger, accusations, and escalation.
So instead of asking, “How do I prove the truth?”
Ask:
“How do I lower distress?”
“How do I keep this person emotionally safe?”
“How do I redirect without humiliating them?”
That is dementia care.
THE MEDICATION TRAP
Now let’s talk about what often happens next.
A caregiver calls the doctor and says:
“She is getting out of hand.”
“She is making accusations.”
“She is yelling.”
“She is screaming.”
“She is worse.”
And too often, the next response becomes:
“How much medication is she on?”
“Let’s increase it.”
Now listen carefully.
Medication has a place.
There are situations where medication is appropriate. There are situations where symptoms are dangerous, severe, or medically complex and require treatment. These decisions should always be made with qualified clinicians.
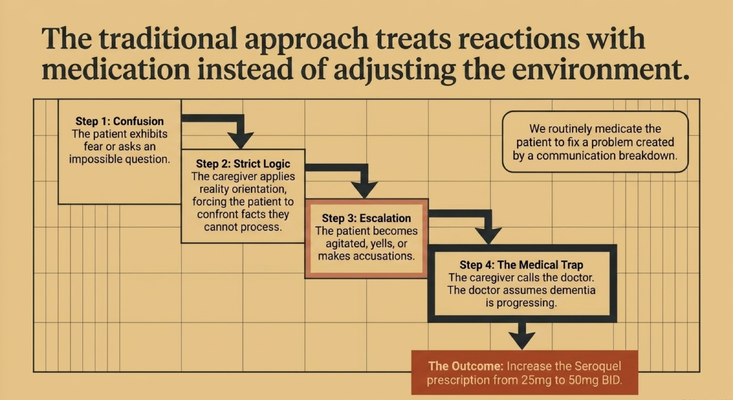
But too often, we medicate a reaction that was created by a communication breakdown.
The person is confused.
The caregiver uses strict logic.
The person becomes agitated.
The doctor hears “agitation.”
Medication gets increased.
And nobody asks:
What happened before the behavior?
What did the caregiver say?
Was the person afraid?
Was the environment confusing?
Was there pain?
Was there hunger?
Was there a shadow?
Was there embarrassment?
Was the person overwhelmed?
That is the trap.
If we do not investigate the root cause, we may treat the reaction instead of solving the problem.
THE NUMBERS SHOW THE SYSTEM IS NOT READY
Now let’s zoom out.
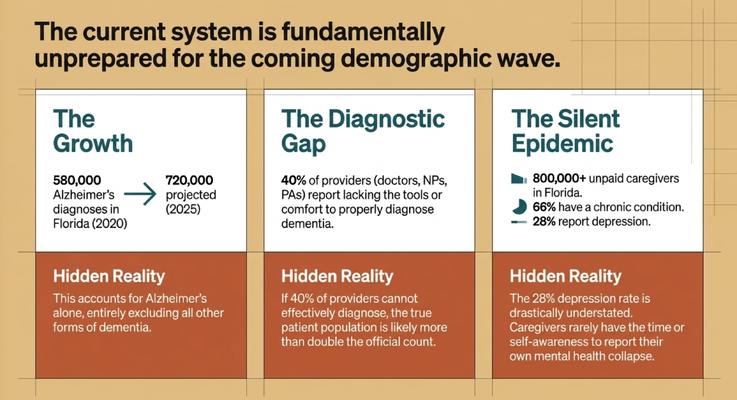
In Florida, there were about 580,000 people diagnosed with Alzheimer’s disease in 2020.
By 2025, that number was projected to be around 720,000.
And remember, that is only Alzheimer’s disease.
Alzheimer’s is not the only type of dementia.
So the true number of people living with dementia is higher.
Now here is another statistic that should make all of us pause:
Around 40% of providers — doctors, nurse practitioners, physician assistants, and others — report that they do not feel comfortable or do not feel they have the right tools to properly diagnose dementia.
So if we already estimate 720,000 people with Alzheimer’s disease in Florida, but a large percentage of providers are uncomfortable making the diagnosis, what does that tell us?
The real number is probably higher.
Much higher.
Then we have caregivers.
In Florida, there are more than 800,000 unpaid caregivers supporting people living with dementia.
Many of them are adult children.
Many are spouses.
Many are still working.
Many have their own health problems.
Around 66% of these caregivers have a chronic condition themselves.
Around 28% report depression.
And I believe that depression number is understated.
Because how many caregivers walk around saying, “Please survey me, I’m depressed”?
Most do not.
They say:
“I’m fine.”
“I have to do this.”
“Nobody else can.”
“I’ll rest later.”
And then their own health starts collapsing.
That is why dementia care cannot only focus on the patient.
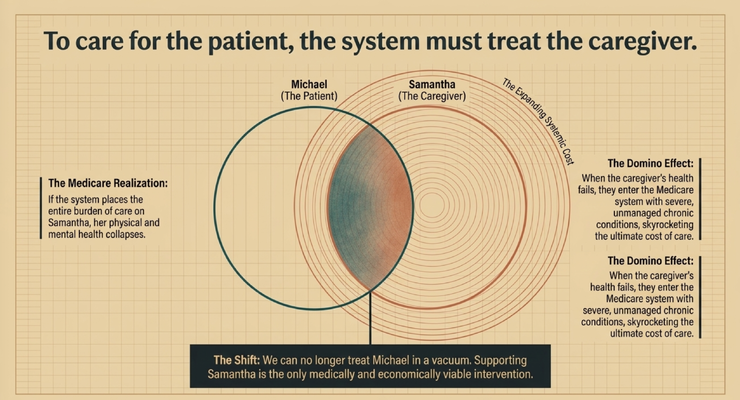
To care for the patient, the system has to support the caregiver.
THE CAREGIVER IS NOT A SIDE ISSUE
Let’s use a simple example.
Michael is the person living with dementia.
Samantha is the caregiver.
If we only treat Michael and ignore Samantha, we are missing the real home care system.
Because Samantha is the one helping with meals.
Samantha is the one managing medications.
Samantha is the one answering repeated questions.
Samantha is the one waking up at night.
Samantha is the one helping with bathing.
Samantha is the one coordinating appointments.
Samantha is the one watching for falls, wandering, confusion, and agitation.
And if Samantha collapses, what happens to Michael?
The whole care environment becomes unstable.
This is the Medicare realization:
You cannot place the entire burden of care on the caregiver and expect the system to survive.
If the caregiver’s physical and mental health fails, the cost of care rises.
But more importantly, the family suffers.
The patient suffers.
The home becomes fragile.
That is why the caregiver is not extra.
The caregiver is part of the care plan.
WHAT THE GUIDE MODEL ACTUALLY IS
This is where the GUIDE Model comes in.
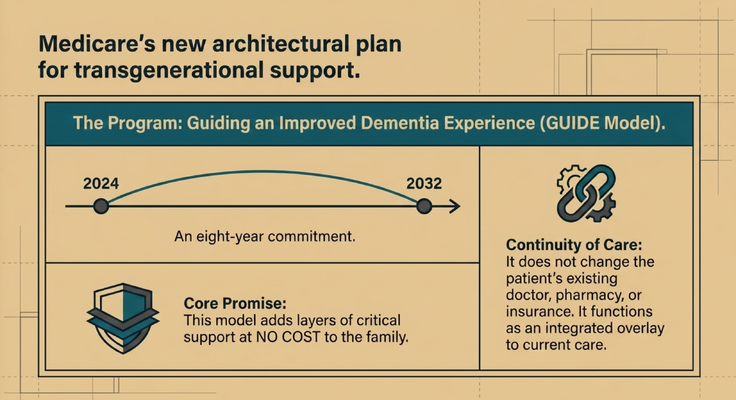
GUIDE stands for Guiding an Improved Dementia Experience.
It is an eight-year Medicare model designed to support people living with dementia and the caregivers helping them at home.
And this is important:
It does not replace the patient’s doctor.
It does not replace the pharmacy.
It does not replace the insurance.
It functions as an added layer of dementia-care support around the family.
For families, that matters.
Because caregivers do not need another disconnected piece of paper.
They need navigation.
They need someone who can help them understand what is happening.
They need someone who can help them think through behaviors, respite, support groups, care coordination, and safety.
They need someone who can say:
“Let’s slow down. Let’s figure out what is really going on.”
That is the shift.
From medication alone to navigation.
From crisis reaction to guided support.
From the patient alone to the patient and caregiver together.
WHO QUALIFIES FOR GUIDE?
Families often ask:
“Dr. Erik, who is this program actually for?”
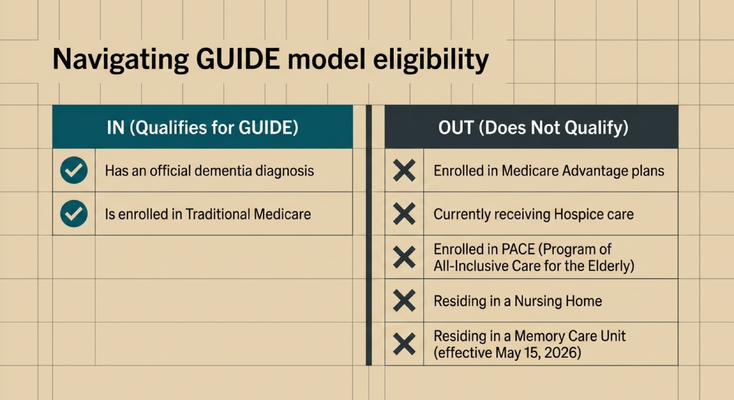
In simple terms, the person needs an official dementia diagnosis and Traditional Medicare.
The program generally does not apply if the person is enrolled in Medicare Advantage, is currently receiving hospice care, is enrolled in PACE, or is residing in a nursing home. And as of May 15, 2026, memory care unit residence affects eligibility as well.
This is why eligibility has to be reviewed carefully.
Every family’s situation is different.
But the bigger point is this:
If you are caring for someone living with dementia, do not assume you have to figure everything out alone.
Ask.
Check eligibility.
Get clarity.
Because many families do not even know this support exists.
RESPITE REBUILDS CAREGIVER CAPACITY
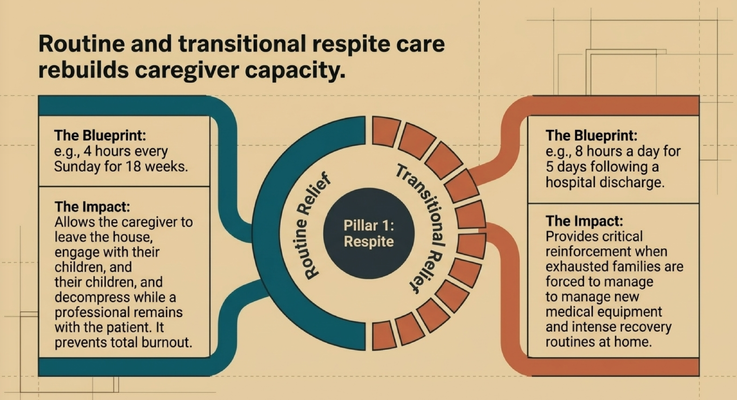
One of the most important parts of the GUIDE Model is respite.
And I want to explain respite in plain language.
Respite means the caregiver gets a break.
Not because the caregiver does not love the person.
Not because the caregiver is abandoning the person.
Because the caregiver is human.
Imagine Samantha is caring for her mother every day.
She loves her mother.
She wants her safe.
But she has children.
She has a spouse.
She has a body.
She has a brain.
She has her own health.
What if every Sunday for four hours, someone could be with Mom while Samantha leaves the house, spends time with her family, decompresses, or simply breathes?
That can prevent burnout.
Or imagine Mom comes home after a hospital discharge.
Now there is a hospital bed.
New instructions.
New equipment.
New weakness.
New anxiety.
New routines.
And Samantha is exhausted.
What if, for a short transitional period, support could come into the home to help during that fragile post-discharge window?
That is not a luxury.
That is capacity rebuilding.
Because if the caregiver breaks, the whole system breaks.
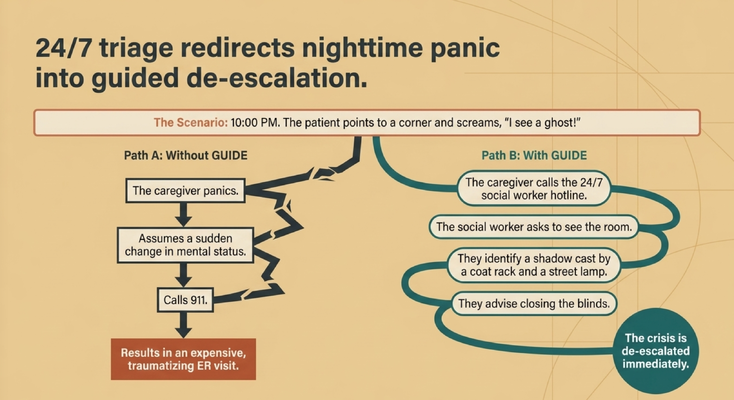
THE 10 PM PROBLEM
Now let’s talk about what happens at night.
It is 10 PM.
Mom looks toward the corner of the room and screams:
“I see a ghost!”
What does the caregiver do?
Without support, the caregiver may panic.
They may assume there is a sudden change in mental status.
They may call 911.
The family may end up in the emergency room.
And sometimes, yes, an emergency evaluation is necessary. If there is sudden confusion, severe symptoms, danger, fall, infection concern, stroke-like symptoms, or anything medically urgent, you seek help.
But sometimes the problem is environmental.
Maybe the blinds are open.
Maybe a streetlight is casting a shadow.
Maybe there is a coat rack in the corner.
Maybe the dementia brain is misinterpreting what it sees.
A trained person on a helpline can slow the situation down.
“Show me the room.”
“Where is she pointing?”
“Is there a shadow?”
“Can you close the blinds?”
“Can you move the coat rack?”
“Can you sit with her and reassure her?”
That can turn panic into de-escalation.
And this is the kind of support caregivers need.
Not judgment.
Not “good luck.”
Guidance.
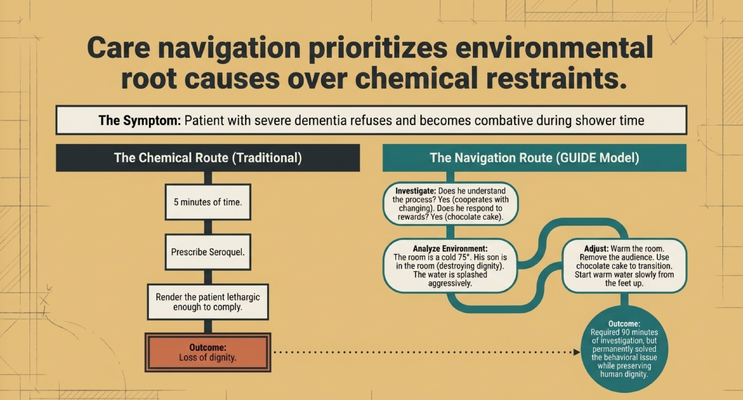
SHOWER REFUSAL IS NOT ALWAYS “JUST DEMENTIA”
Another example I spoke about is shower refusal.
A person living with severe dementia refuses to shower and becomes combative.
There are two ways to approach that.
The fast route is to medicate.
Make the person sedated enough to comply.
But what is the outcome?
Loss of dignity.
The better route is to investigate.
I remember a case where the person had severe dementia and refused the shower. But when he soiled himself, he could still stand and allow someone to change him.
That told us something very important.
He could still understand parts of the care process.
So the question became:
What is different about the shower?
Was the room cold?
Was the water being splashed too aggressively?
Was he embarrassed?
Was his son in the room?
Was privacy being protected?
Was the caregiver rushing?
Were the clothes, towels, water, lighting, and tone prepared?
We found the issue.
It was not “just dementia.”
It was the shower environment.
So we changed the approach.
Warm the room.
Protect dignity.
Remove unnecessary people from the room.
Use chocolate cake as a positive motivator.
Introduce water slowly from the feet upward.
Speak calmly.
Move with patience.
That took much longer than writing a prescription.
But it solved the real problem.
That is dementia care.
Not just controlling behavior.
Understanding behavior.
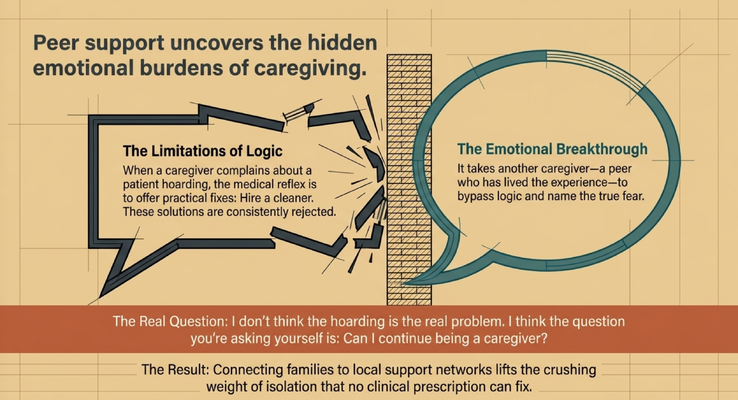
THE POWER OF PEER SUPPORT
I am a big believer in support groups.
And I want to tell you why.
I once sat in a support group where a caregiver was talking about her husband hoarding things. She was frustrated. She was overwhelmed. She kept describing the clutter.
My doctor brain went straight to logic.
“Hire someone to clean.”
“Try this.”
“Try that.”
Every suggestion was rejected.
Then another caregiver in the room said something different.
She said:
“I don’t think the hoarding is the real problem. I think the real question you’re asking yourself is: can I continue being a caregiver?”
And the room stopped.
The caregiver started crying.
Because that was the truth underneath the complaint.
The hoarding was the surface issue.
The deeper issue was fear.
Exhaustion.
Guilt.
The question of whether she could continue caring for the person she loved.
That is the power of peer support.
Sometimes another caregiver can say what the doctor cannot see.
Sometimes another caregiver can name the emotional burden faster than any clinical checklist.
That is why connecting families to support groups matters.
Because no medication can fix isolation.
THE GUIDE MODEL IS NOT JUST A CHECK-IN
At the end of the talk, I shared something that happened after I spoke at the World Health Expo.
I had been on stage with major healthcare organizations. Big room. Big event. Thousands of people.
But the moment that stayed with me was not the stage.
It was one caregiver.
A woman came up to me and said:
“Dr. Erik, my mom is in your GUIDE Model program. Irina, the care navigator, has been a lifesaver for us.”
That is what matters.
Not the stage.
Not the title.
Not the applause.
The family.
The caregiver.
The person living with dementia.
The life that is actually being changed.
Under the GUIDE Model, there are required touchpoints. But I tell my team all the time:
It is not about the phone call.
It is about what happens inside that call.
Did you leave the caregiver with something valuable?
Did you remind them to discuss advance directives?
Did you help them think through respite?
Did you identify a safety issue?
Did you connect them to support?
Did you reduce panic?
Did you help them feel less alone?
A call can be transactional.
“Hello, how are you? Everything okay? Great. Click.”
That is not enough.
Dementia care has to be more than checking a box.
It has to change lives.
WHAT I WANT CAREGIVERS TO REMEMBER
If you are caring for someone living with dementia, here is what I want you to take from this:
Do not argue with dementia reality.
Validate first.
Redirect second.
Do not assume every behavior means the dementia is simply getting worse.
Ask what happened before the behavior.
Look at the environment.
Look at pain.
Look at fear.
Look at dignity.
Look at lighting.
Look at routine.
Look at caregiver exhaustion.
And please remember:
You are part of the care plan.
Your health matters.
Your sleep matters.
Your depression matters.
Your chronic conditions matter.
Your ability to continue matters.
You are not weak because you need support.
You are human.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why the GUIDE Model matters.
Through the GUIDE Model — Guiding an Improved Dementia Experience — eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Medicare-covered respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because dementia care is not only about medication.
It is about navigation.
It is about dignity.
It is about caregiver support.
It is about understanding behaviors before escalating medications.
It is about helping families stay steady inside a disease that can feel chaotic.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, caregiver support, the GUIDE Model, validation, respite, and practical strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia symptoms, medication changes, hallucinations, agitation, shower refusal, caregiver burnout, respite needs, safety concerns, and eligibility for care programs should be discussed with qualified healthcare professionals. If symptoms are severe or urgent, seek immediate medical help.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health