THE EXPECTATION VERSUS THE REALITY
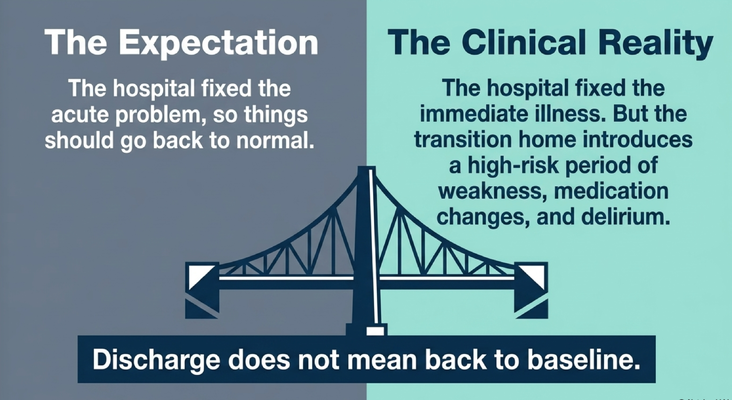
The expectation is simple.
Your loved one goes into the hospital. The hospital finds the problem. The hospital treats the problem. Then your loved one comes home, and everything goes back to normal.
That is what we all hope for.
But the clinical reality is more complicated.
The hospital may fix the immediate illness, but the transition home can introduce a high-risk period of weakness, medication changes, delirium, sleep disruption, anxiety, and functional decline.
That is especially true for a person living with dementia.
Why?
Because dementia lowers the brain’s ability to handle stress. A younger, healthier person may go to the hospital, lose sleep, have medications adjusted, feel weak for a few days, and recover. But a person living with dementia may not have the same cognitive reserve.
The brain is already vulnerable.
So when you add infection, pain, anesthesia, unfamiliar staff, alarms, interrupted sleep, new medications, stopped medications, immobility, and a disrupted routine, the whole system can destabilize.
That is why I tell families:
Do not assume discharge means the crisis is over.
For dementia families, discharge is often the beginning of the next care plan.
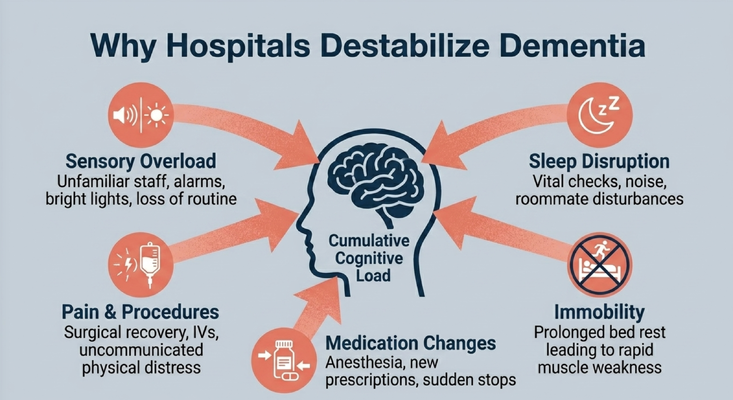
WHY THE HOSPITAL CAN DESTABILIZE DEMENTIA
Let’s put ourselves in the shoes of the person living with dementia.
They are 85 years old. They have dementia. They are used to their home, their chair, their bedroom, their bathroom, their routine, their caregiver, their lighting, their sounds.
Then suddenly, they are in the hospital.
Unfamiliar staff are walking in and out. Alarms are going off. Lights are bright. There are new voices, new rooms, new routines, new medications, and sometimes a roommate who is also confused, in pain, or calling out.
Then the sleep disruption begins.
Vital signs at night. Blood pressure checks. Blood draws. IVs. Procedures. Pain. Noise. Roommate disturbances. Doctors and nurses coming in at different times.
When I was a resident physician, there were times we had to do procedures at 3 AM. Sometimes that is medically necessary. But think about what that feels like to a person living with dementia.
They are sleeping, confused, disoriented, and suddenly someone they do not know is coming in to do something painful or frightening.
Now add immobility.
A person comes in walking, but then they spend days in bed because of pneumonia, a fall, surgery, or weakness. The longer they stay in bed, the more muscle weakness they can develop. And the harder it can be to get them back to baseline.
That is why one of the most important questions you can ask in the hospital is:
“How soon is it safe to get them out of bed and into the chair?”
And then:
“How soon can they work with physical therapy?”
Out of bed into the chair. Out of the chair into walking when safe. That matters.
Because mobility is medicine.
And finally, medication changes.
New prescriptions. Stopped medications. Adjusted medications. Old medication lists. Polypharmacy — which simply means too many medications at one time. All of this can create confusion, dizziness, sedation, constipation, urinary retention, sleep disruption, or falls.
So if your loved one comes home different, do not jump straight to:
“The dementia just got worse.”
Ask:
“What happened during the hospitalization?”
MEDICALLY STABLE IS NOT THE SAME AS FUNCTIONALLY SAFE
This is one of the most important ideas in post-hospital dementia care.
The hospital may say:
“The infection is treated.”
“The vitals are stable.”
“The wound is healing.”
“The labs are improving.”
“She is cleared for discharge.”
And all of that may be medically true.
But when the family gets home, the caregiver may see a completely different reality.
Mom is weaker.
Dad cannot get to the bathroom safely.
There is new incontinence.
There is more anxiety.
There is fragmented sleep.
There are medication side effects.
There is loss of routine.
There is confusion that worsens at night.
There is a caregiver staring at a discharge packet thinking, “I do not know what I am supposed to do with all of this.”
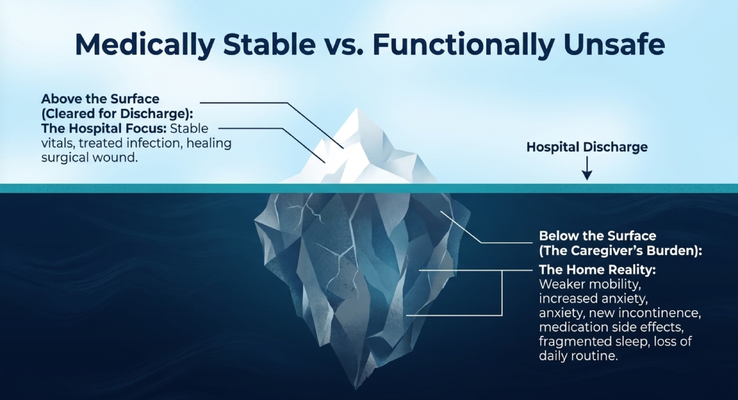
That is the iceberg.
Above the surface is what the hospital focused on: stable vitals, treated infection, healing wound.
Below the surface is the home reality: mobility decline, medication confusion, caregiver burden, safety risks, sleep disruption, anxiety, and loss of daily function.
And that below-the-surface reality is where caregivers live.
So before you leave the hospital, it is okay to ask the hard questions.
Actually, you should ask them.
“Is my loved one safe to discharge home?”
“Do we have the equipment we need?”
“Can they transfer safely?”
“Can they use the bathroom safely?”
“Do we need a walker, shower chair, commode, hospital bed, or home health?”
“What changed with the medications?”
“What should I watch for tonight?”
“Who do I call if confusion worsens?”
I know those conversations can feel uncomfortable. You may feel like you are putting the doctor, nurse, or case manager on the spot.
But what do I always say?
It is better to have difficult conversations than to be in difficult situations.
THE TWO BIG POST-DISCHARGE VULNERABILITIES
There are two post-discharge vulnerabilities I want every caregiver to understand.
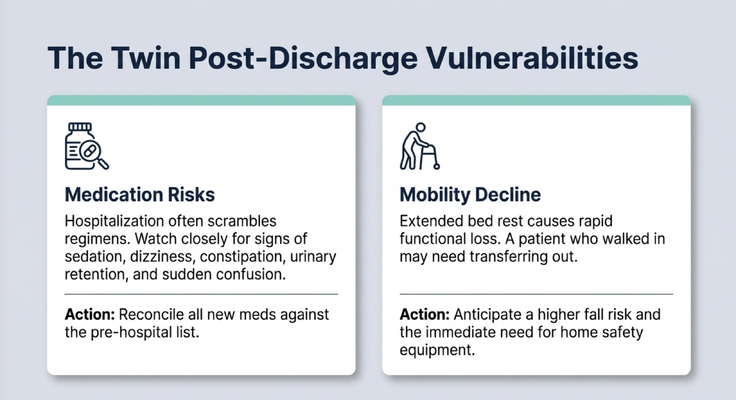
The first is medication risk.
Hospitalization often scrambles medication regimens. A medication may be started. Another may be stopped. Another may be adjusted. Sometimes the hospital has an old medication list. Sometimes the family forgets to bring the current list. Sometimes a medication that was being taken at home is accidentally missed.
This can be dangerous.
Watch closely for sedation, dizziness, constipation, urinary retention, sudden confusion, increased falls, or a change in alertness.
And please remember: do not stop or restart medications on your own without medical guidance. Certain medications, especially sedatives or psychiatric medications, can be risky to stop suddenly. If something looks wrong, call the medical team and ask for clarification.
The action step is simple:
Reconcile the medication list.
That means comparing the medications your loved one was taking before the hospital with the medications they are being told to take after the hospital.
Ask:
“What was started?”
“What was stopped?”
“What was changed?”
“What is temporary?”
“What should continue?”
“What side effects should I watch for?”
The second vulnerability is mobility decline.
Extended bed rest can cause rapid functional loss. A person who walked into the hospital may come home needing help transferring, standing, toileting, or walking.
That means the fall risk may be higher than before.
So do not wait for the fall to happen.
Ask about physical therapy. Ask about home safety. Ask whether equipment is needed. Ask whether the person can safely transfer from bed to chair, chair to toilet, and toilet back to standing.
A smooth discharge is not only about paperwork.
It is about whether the person can function safely in the home.
THE CAREGIVER TAKES OVER OVERNIGHT
Now let’s talk about the caregiver.
Because once the hospital doors close, the caregiver suddenly becomes the care coordinator, medication manager, safety monitor, sleep monitor, transportation coordinator, advocate, and emotional support system.
That is a lot.
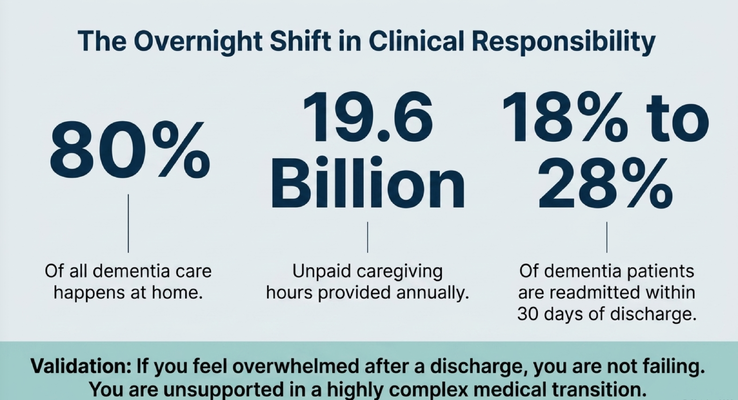
And most dementia care already happens at home.
So who is home?
The caregiver.
People like my mom and dad, who are around 70 years old and taking care of my grandmother, who is 93. They are managing their own health while caring for someone they love.
That is real life.
And if you are a caregiver reading this after a hospital discharge and you feel overwhelmed, I want you to hear me clearly:
You are not failing.
You are unsupported in a highly complex medical transition.
That is different.
You may be dealing with new medications, new weakness, new confusion, new equipment, new instructions, new follow-up appointments, and new behaviors all at the same time.
And then people wonder why caregivers are exhausted.
This is why support matters.
This is why discharge planning matters.
This is why the caregiver should not be treated like a side note.
In dementia care, the caregiver is part of the care plan.
If the caregiver collapses, the whole home care environment becomes fragile.
DR. ERIK’S 5 POST-HOSPITAL QUESTIONS
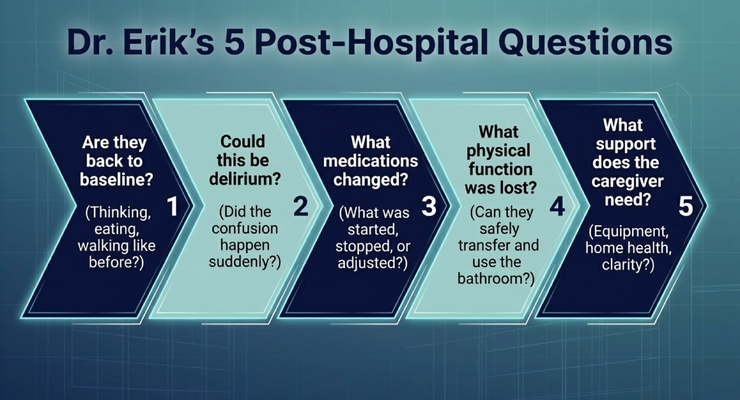
Here are the five questions I want every caregiver to ask after a hospital stay.
Question one:
Are they back to baseline?
Not just medically. Functionally.
Are they thinking the way they were thinking before?
Are they eating the way they were eating before?
Are they walking the way they were walking before?
Are they sleeping the way they were sleeping before?
Can they get to the bathroom?
Can they transfer safely?
If the answer is no, then something changed.
Question two:
Could this be delirium?
If confusion happened suddenly, over hours or days, do not assume it is just dementia progression.
Dementia usually progresses gradually. Delirium is sudden and can fluctuate. It can be triggered by infection, dehydration, pain, constipation, medication changes, hospitalization, surgery, poor sleep, or another acute medical issue.
So if your loved one is suddenly more confused, more sleepy, more agitated, hallucinating, or not themselves, ask the medical team:
“Could this be delirium?”
Question three:
What medications changed?
This is the glue that holds everything together.
What was started?
What was stopped?
What was adjusted?
What was temporary?
What was missed?
What side effects should we watch for?
What interactions are possible?
Bring the old list and the new list together. Ask the doctor, pharmacist, or qualified medical professional to review them with you.
Question four:
What physical function was lost?
Can they safely stand?
Can they transfer?
Can they use the bathroom?
Can they walk to the kitchen?
Can they feed themselves?
Can they use their hands the same way?
Can they get in and out of bed?
Function matters. A person may be medically stable but unsafe at home without support.
Question five:
What support does the caregiver need?
This is not optional.
If you are on an airplane and the oxygen mask drops, what do they tell you?
Put your own mask on first.
Why?
Because if you cannot breathe, you cannot help the person next to you.
Dementia caregiving works the same way.
What equipment do you need?
Do you need home health?
Do you need respite?
Do you need help understanding the discharge instructions?
Do you need someone to walk through the medication changes?
Do you need someone to call if things worsen at night?
These are not selfish questions.
These are safety questions.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why caregivers should not have to navigate dementia care alone.
Through the GUIDE Model — Guiding an Improved Dementia Experience — eligible families may receive structured dementia-care support through MedBetter Health.
MedBetterHealth.org is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Up to $2,500 respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters after a hospital discharge.
Because the caregiver may need help understanding medication changes.
They may need help knowing whether sudden confusion could be delirium.
They may need help thinking through respite.
They may need help knowing what to ask the doctor.
They may need help watching for warning signs.
They may need help building a safer home transition.
A discharge packet is not a dementia care plan.
Families need support after the hospital doors close.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetterHealth currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetterHealth remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, hospital discharge, delirium, caregiver support, and practical care strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Hospital discharge decisions, medication changes, delirium, sudden confusion, falls, weakness, infection symptoms, pain, caregiver burnout, equipment needs, and safety concerns should be discussed with qualified healthcare professionals. If symptoms are severe or urgent, seek immediate medical help.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health