THE TIMELINE: 30 YEARS OF DEMENTIA PHARMACOLOGY
Here is what the history of dementia treatment actually looks like:
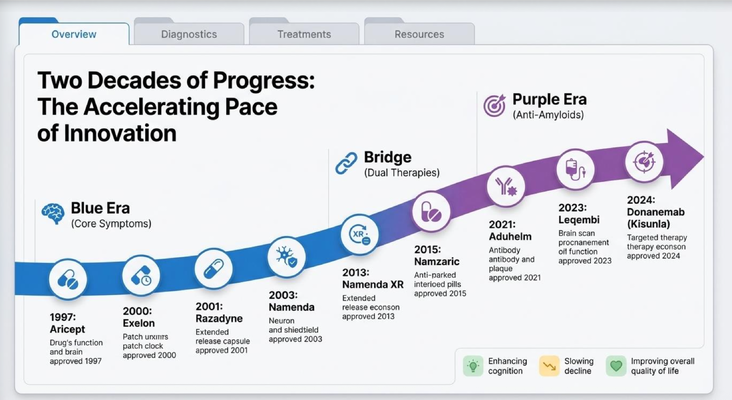
1997 — Aricept (donepezil) came out. Still one of the most commonly prescribed drugs in dementia today, nearly 30 years later.
2000 — Exelon (rivastigmine) , a transdermal patch. Same mechanism as Aricept — preserving acetylcholine — just delivered differently.
2001 — Razadyne (galantamine) , extended-release capsule. Same family of drugs.
2003 — Namenda (memantine) came out. A different type entirely — it works on glutamate, not acetylcholine. Prescribed for moderate to severe Alzheimer's.
Then from 2003 to 2013 — honestly, not a lot of new things happened. The biggest change was that we took Namenda and made it extended-release: Namenda XR. In 2015 we combined Aricept and Namenda into one pill — Namzaric. Useful, but not revolutionary.
That was the state of dementia treatment for nearly two decades.
THE PARADIGM SHIFT: A NEW ERA BEGINS
Here is where things get genuinely interesting.
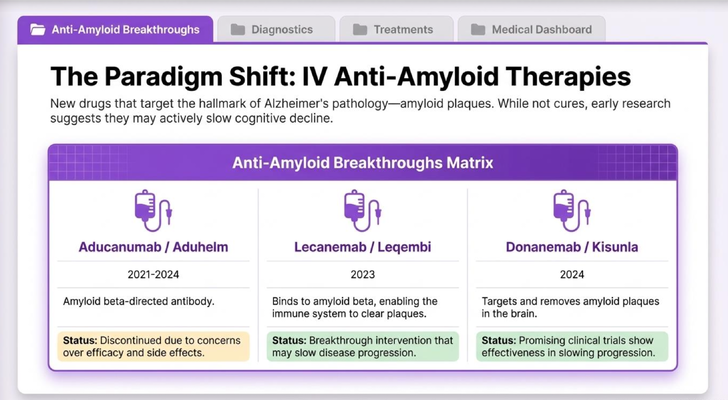
The classic medications — Aricept, Namenda, all of them — they work on neurotransmitters. They try to preserve the chemicals in your brain that help with memory and cognition. What they do not do is go after the actual cause of Alzheimer's disease: the amyloid plaques building up in the brain.
The theory, which we are now testing with real data, is this: if we can remove those plaques, we can slow how fast the disease progresses.
That is the paradigm shift.
2021 — Aduhelm (aducanumab) was the first attempt. Unfortunately, it was discontinued due to concerns over efficacy and side effects. We are no longer using it.
2023 — Leqembi (lecanemab) — this is a breakthrough. An IV infusion that binds to amyloid beta and helps your immune system clear the plaques. Clinical data shows it may meaningfully slow disease progression. This is the real deal.
2024 — Kisunla (donanemab) — promising clinical trials show effectiveness in slowing progression. Still relatively new, but the data is encouraging.
These are not cures. I want to be clear about that. Your loved one is not going to get their memory back. But slowing progression — buying time, preserving function longer — that is significant.
THE SIDE EFFECT YOU NEED TO KNOW ABOUT: ARIA
These new IV drugs come with a side effect called ARIA — Amyloid-Related Imaging Abnormalities. It sounds intimidating, but here is what it means in plain language.
When your immune system starts clearing the plaques from around the brain's blood vessels, two things can sometimes happen: a small amount of bleeding (hemorrhage) or a small amount of swelling (edema).
That is why patients on these drugs need regular MRI scans — to monitor for these changes and catch them early if they appear.
My advice: do not let this automatically scare you off. Have a real conversation with your neurologist. Ask: what is my specific risk of ARIA? What are the actual benefits for my loved one's stage of disease? How much can we realistically slow the progression? These are the right questions.
THE SUPPORTING CAST: SECONDARY MEDICATIONS
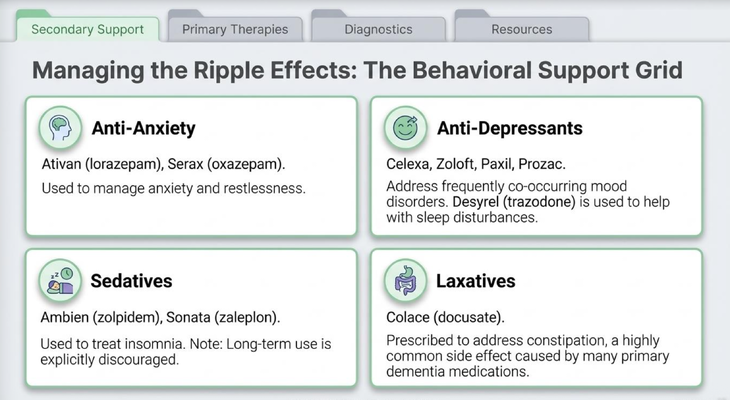
Beyond the cognitive drugs, there is a whole category of medications that manage the symptoms that come alongside dementia:
Anti-anxiety medications — Ativan (lorazepam), Serax (oxazepam). Used to manage anxiety and restlessness.
Antidepressants — Celexa, Zoloft, Paxil, Prozac. Depression is extremely common in dementia. Desyrel (trazodone) is also used specifically for sleep disturbances.
Sedatives — Ambien (zolpidem), Sonata (zaleplon) for insomnia. Important note: long-term use is explicitly discouraged.
Laxatives — Colace (docusate). Constipation is one of the most common side effects of primary dementia medications and is frequently undertreated.
THE ONE CATEGORY THAT REQUIRES EXTREME CAUTION
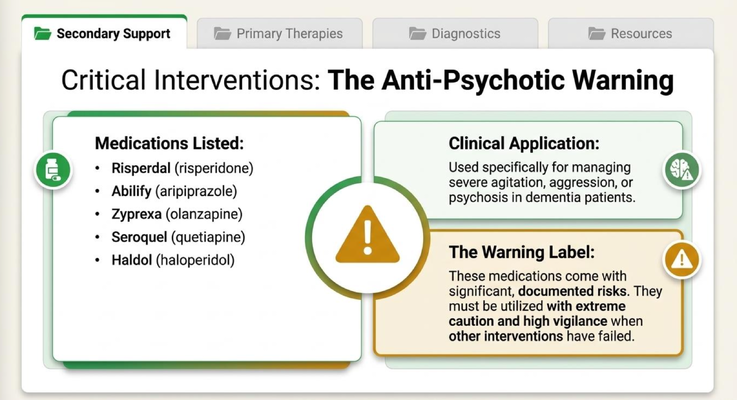
Anti-psychotics — Risperdal, Abilify, Zyprexa, Seroquel, Haldol — are sometimes prescribed for severe agitation, aggression, or psychosis in dementia patients.
These medications come with significant, documented risks. They must be used with extreme caution, under close supervision, and only when other interventions have failed.
If a doctor recommends an anti-psychotic for your loved one, do not panic — but do ask questions. Ask why, what the risks are, what alternatives were considered, and what the monitoring plan looks like. You have every right to that conversation.
The Invisible Epidemic: Caregiver Confusion
Most caregivers I speak to have no idea that drugs like Leqembi even exist. They are managing their loved one's medications one prescription at a time, without a full picture of what is available, what is new, or what questions they should be asking.
That is not a failure on their part. It is a system problem. And it is exactly why the GUIDE Model exists.
The GUIDE Model: Medicare's New Dementia Care Program
MedBetter Health is proud to participate in Medicare's GUIDE Model — Guiding an Improved Dementia Experience. This 8-year CMS initiative is transforming dementia care nationwide.
Through the program, eligible beneficiaries and their caregivers receive:
A dedicated Care Navigator who coordinates all aspects of care Monthly support calls and 24/7 helpline access Medicare-covered respite care so caregivers can get the break they need Caregiver education and training Personalized dementia care plans and social needs screening
If you have traditional Medicare and a confirmed dementia diagnosis, you may be eligible.
👉 Check your eligibility for the GUIDE Model Program in under two minutes: https://medbetterhealth.org/guide
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting every caregiver with practical, evidence-based education.
Straight Talk With Dr. Erik

Learn more about dementia. Watch the full video and subscribe for regular insights.
https://www.youtube.com/@ErikIlyayev
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health