PARANOIA IS PART OF THE DISEASE PROCESS
Let’s start with something important.
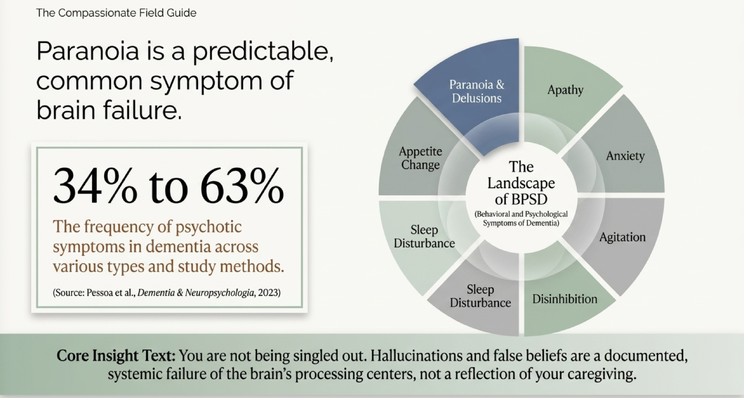
Paranoia and false beliefs are common in dementia.
In the presentation, I talked about psychotic symptoms in dementia occurring in roughly 34% to 63% of cases, depending on the dementia type and study method. These symptoms can include paranoia, delusions, hallucinations, agitation, anxiety, sleep disturbance, disinhibition, and appetite changes.
Clinically, these are part of what we call BPSD — behavioral and psychological symptoms of dementia.
I want caregivers to remember that phrase because it matters.
Behavioral and psychological symptoms of dementia.
These are not random personality problems. These are not your loved one “choosing” to hurt you. These are not proof that you are failing as a caregiver.
These symptoms come from changes in the brain.
So when your loved one accuses you of stealing, lying, cheating, abandoning them, or trying to control them, the first thing I want you to do is this:
Do not take it personally.
I know that is easier said than done.
But if you take every accusation as a personal attack, you will spend your caregiving life defending yourself inside a reality your loved one’s brain can no longer process correctly.
That is exhausting.
And it does not work.
THEIR REALITY IS NOT YOUR REALITY
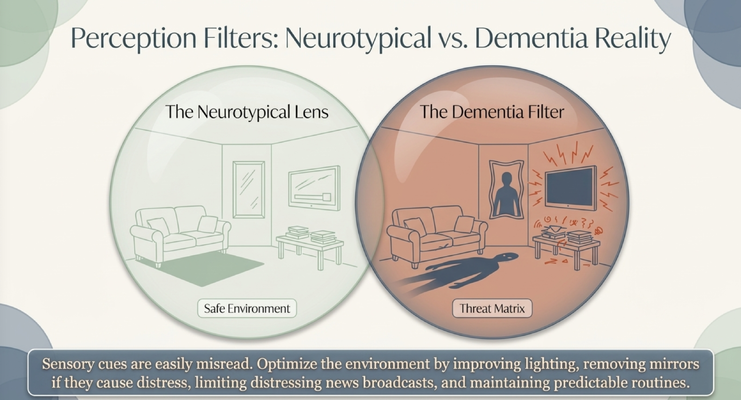
One of the hardest parts of dementia care is accepting that two people can be standing in the same room and experiencing two completely different realities.
You may walk into the living room and see a couch, a table, a mirror, and the television.
Your loved one may walk into that same room and see something threatening.
Maybe a shadow looks like a person.
Maybe a mirror reflection looks like a stranger.
Maybe a sound from the television feels like danger.
Maybe a normal object on the table looks unfamiliar, frightening, or suspicious.
This is what I mean when I say the dementia brain can misread sensory cues.
The environment may look safe to you, but to your loved one, it may feel unsafe.
That is why arguing the facts often fails.
You are arguing from your reality.
They are reacting from theirs.
You may say, “There is no one in the mirror.”
But if their brain is showing them a person in the mirror, your correction does not comfort them. It may actually make them feel more alone, more confused, and more defensive.
The goal is not to force them to see what you see.
The goal is to lower the fear.
That might mean improving lighting, removing mirrors if they cause distress, reducing frightening television or news, keeping routines predictable, limiting overstimulation, and making the environment easier for the brain to understand.
Sometimes the intervention is not a medication.
Sometimes it is turning off the news, closing the blinds, moving a mirror, or turning on a lamp before shadows start creating problems.
SUDDEN PARANOIA IS A RED FLAG
Now, there is a very important distinction caregivers need to understand.
If your loved one has gradually developed paranoia over time, that may be part of the dementia progression.
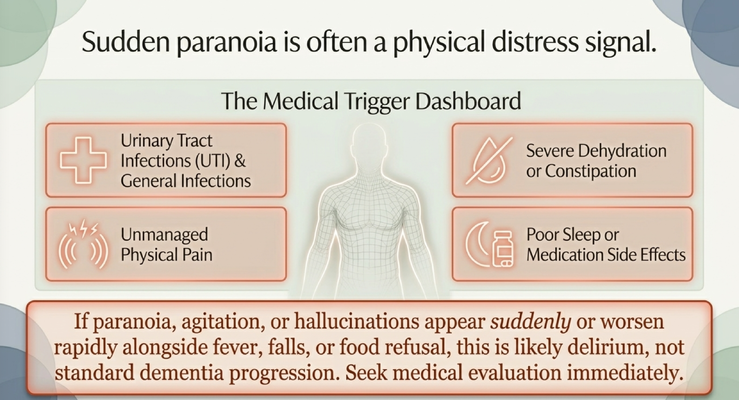
But if paranoia appears suddenly, or if it gets dramatically worse within 24 to 48 hours, do not simply say, “That’s just the dementia.”
Sudden change is a red flag.
If someone was relatively stable and now suddenly becomes paranoid, agitated, hallucinating, aggressive, confused, or very different from baseline, we have to think medically.
Could this be a urinary tract infection or another infection?
Could they be dehydrated?
Could they be constipated?
Could they be in pain?
Could they have poor sleep?
Could this be a medication side effect?
Could there be an electrolyte problem?
Could this be delirium?
This matters because delirium and acute medical problems can look like dementia worsening, but they require a different response.
Your loved one may not be able to say, “I am in pain.”
They may not be able to say, “I have not gone to the bathroom in five days.”
They may not say, “I feel burning when I urinate.”
They may not say, “This new medication is making me feel strange.”
Instead, the body speaks through behavior.
So when paranoia, hallucinations, agitation, or accusations appear suddenly, treat that as a medical warning sign. Call the doctor. Report the change clearly. Ask about infection, dehydration, pain, constipation, sleep disruption, medication changes, or other acute causes.
Dementia progression is usually gradual.
A sudden drop deserves medical attention.
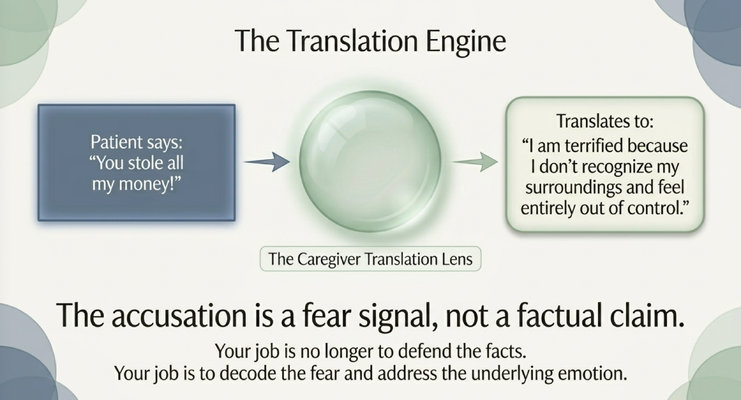
THE ACCUSATION IS A FEAR SIGNAL
Now let’s talk about the accusation itself.
When your loved one says, “You stole my money,” they may not actually be communicating, “I have objectively reviewed the facts and concluded that you stole from me.”
What they may really be saying is:
“I am terrified because I do not recognize my surroundings.”
“I cannot find something important.”
“I feel out of control.”
“I do not understand what happened.”
“I feel unsafe.”
That is the translation.
The accusation is a fear signal, not a factual claim.
Let’s use the wallet example.
Your loved one puts the wallet in a drawer. Later, they forget they put it there. Now the wallet is missing from where they expected it to be.
Their brain has a gap.
The brain does not like gaps.
So it tries to fill the gap with the most available explanation.
“She took it.”
“He stole it.”
“They are hiding it from me.”
To us, that explanation is wrong. But to the dementia brain, it may feel completely real because the person cannot retrieve the missing memory.
This is why defending the facts usually fails.
You are trying to solve a memory gap with evidence.
But the person is experiencing fear.
And fear does not calm down just because you present facts.
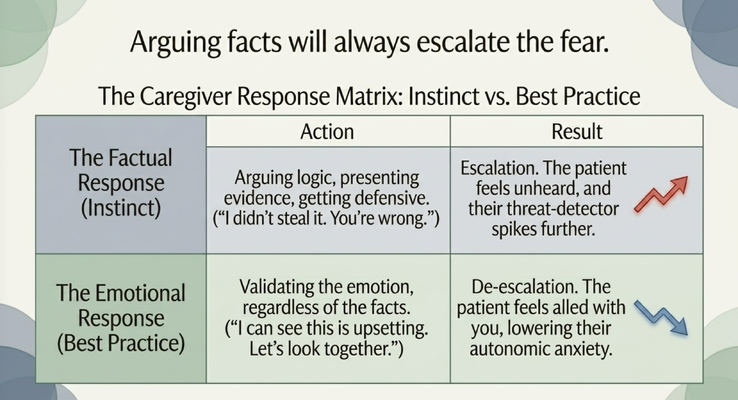
ARGUING FACTS WILL ESCALATE THE FEAR
This is where caregivers often make the mistake that creates the biggest blow-up.
The person says, “You stole my wallet.”
The caregiver says, “I did not steal your wallet. You’re wrong. Why would I do that? I do everything for you.”
That response is understandable.
But it usually escalates the situation.
Why?
Because now your loved one feels unheard.
Their threat detector goes higher.
They feel dismissed. They feel attacked. They feel like you are denying the reality they are experiencing. And the more you defend yourself, the more suspicious they may become.
Think about it this way.
If you were watching me right now and someone walked into the room and said, “You are not watching Dr. Erik. That is not happening,” what would you do?
You would argue.
You would say, “Yes, I am. I can see him right here.”
That is what happens to your loved one.
Their experience feels real to them.
So when you argue against it, you are not calming them down.
You are threatening their reality.
That is why the caregiver’s instinct and the caregiver’s best practice are often different.
The instinct is to defend the truth.
The best practice is to validate the emotion.
Instead of saying, “I didn’t steal it. You’re wrong,” try something like:
“I can see this is really upsetting.”
“I know you’re scared.”
“Let’s look together.”
“I’m here with you.”
You are not agreeing that you stole the wallet.
You are agreeing that they feel scared, unsafe, or distressed.
That is very different.
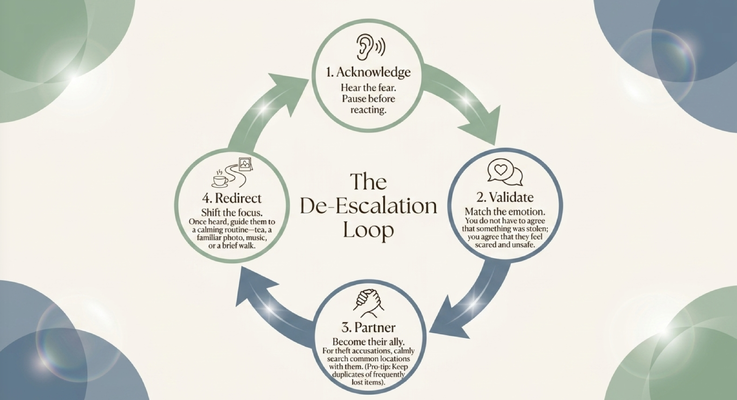
THE DE-ESCALATION LOOP
So what do we do in the moment?
I want you to remember this loop:
Acknowledge.
Validate.
Partner.
Redirect.
First, acknowledge. Hear the fear before you react. Pause. Do not jump immediately into defense mode. Take a breath and recognize that your loved one is distressed.
Second, validate. You do not have to agree with the false belief. You validate the emotion underneath it. You might say, “I can see this is upsetting,” or “I know this feels scary,” or “I hear you, Mom. I understand you’re worried.”
That alone can lower the intensity.
Third, partner. Become their ally instead of their opponent. If the accusation is about a missing item, calmly search common places together. “Let’s look together.” “Maybe it’s nearby.” “I’ll help you find it.”
Now you are on the same side.
Fourth, redirect. Once the emotion has softened, shift attention toward something familiar and calming. Look at family photos. Put on music they love. Offer a snack. Talk about a comforting memory. Move into a safer emotional space.
Maybe you say, “Mom, look at this picture of the grandchildren.”
Or, “Remember this song you and Dad used to dance to?”
Or you put on familiar music and let the brain move away from the accusation.
The goal is not to win the argument.
The goal is to help them feel safe.
WHAT THIS FEELS LIKE FOR THE CAREGIVER
I want to pause here because caregivers need to be seen in this conversation too.
Being accused by someone you love is painful.
You are already doing so much.
You are managing appointments, medications, meals, bathing, transportation, bills, sleep disruption, repeated questions, and family stress. You may be exhausted. You may be trying to do the right thing every single day.
And then the person you are caring for says, “You stole from me.”
That can feel devastating.
It can also feel embarrassing, especially if they say it in front of other people.
You may worry that others believe it. You may feel judged. You may feel like you have to prove yourself.
But I want you to remember: these accusations are a symptom of the disease process. They are not a measure of your character.
You do not need to stand trial in the middle of the living room.
You need a strategy.
And the strategy is not defense.
The strategy is emotional safety.
WHEN TO GET MEDICAL HELP
There are times when paranoia or accusations require professional support.
If the symptoms are sudden, severe, or rapidly worsening, call the doctor.
If there is fever, falls, food refusal, dehydration, pain, new weakness, a recent medication change, or a sudden change in confusion, seek medical evaluation promptly.
If hallucinations, paranoia, or agitation create danger for the person living with dementia or the caregiver, bring in the medical team.
And if you ever feel unsafe, remove yourself from immediate danger and call for help.
This is education, not medical advice. Medication decisions, psychiatric symptoms, delirium evaluation, and safety concerns should be discussed with a qualified healthcare professional.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly the kind of moment caregivers should not have to navigate alone.
When your loved one accuses you of stealing, or becomes paranoid, or starts seeing things differently, you should not have to rely on Google, random advice, or trial and error.
You need someone who understands dementia.
You need someone who can help you think through:
Is this a sudden medical change?
Is this paranoia from dementia?
Is the environment triggering fear?
How do I respond without escalating?
When do I call the doctor?
How do I protect safety without turning every day into a fight?
That is why Medicare created the GUIDE Model — Guiding an Improved Dementia Experience.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Up to $2,500 in respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
This matters because dementia caregiving does not happen only during office hours.
It happens at night.
It happens on weekends.
It happens when mom suddenly gets suspicious.
It happens when dad is agitated.
It happens when you are exhausted and do not know what to say next.
Caregivers need support in the real moments where dementia becomes difficult.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia accusations, paranoia, validation, redirection, and caregiver support by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. If paranoia, hallucinations, agitation, confusion, or accusations appear suddenly or worsen rapidly, speak with a qualified healthcare professional promptly.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health