
THE OLD ERA WAS REACTIVE
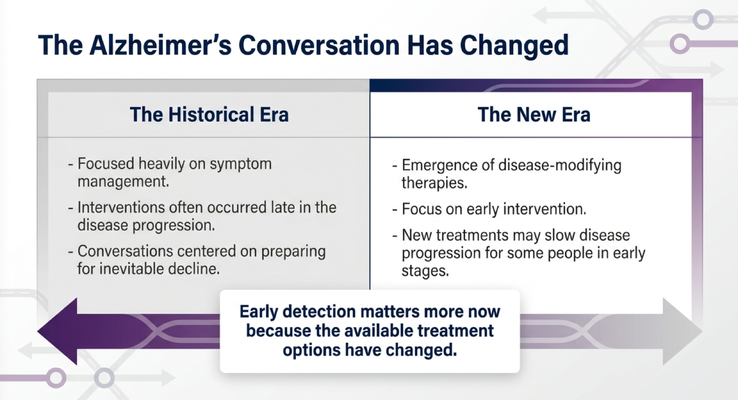
Historically, Alzheimer’s care was mostly reactive.
We focused heavily on symptom management. We waited until the person was clearly struggling. We intervened late in the disease progression. And the conversations often centered around preparing families for inevitable decline.
Now, I want you to understand something.
Alzheimer’s disease does not usually begin the day someone forgets a name or repeats a question.
The disease process can begin many years before the first obvious symptom. Some research suggests Alzheimer’s-related changes may begin 15 years or more before the family notices memory loss.
So if we wait until the symptoms are undeniable, we may already be late.
That was the old era.
It was like the Blockbuster era.
You remember Blockbuster? You had to go to the store, rent the VHS, then the DVD, then bring it back. At the time, that was normal. But eventually the entire model changed.
Then came streaming.
The same kind of shift is happening in Alzheimer’s disease.
For years, we were mostly managing what had already happened. Now, the field is moving toward earlier identification, earlier conversations, earlier planning, and disease-modifying treatment discussions for some people in early stages.
That does not mean we have a cure.
We do not.
But it does mean the timing of diagnosis matters differently now.
THE NEW ERA IS ABOUT TIME
In this new era, there are disease-modifying therapies being studied and used in ways that were not part of the conversation years ago. These therapies are not for everyone, and they are not appropriate at every stage. They require careful clinical evaluation, specialist involvement, discussion of risks and benefits, and the right timing.
But the point is this:
If someone is diagnosed too late, the window for certain treatment discussions may already be closed.
That is why early detection matters.
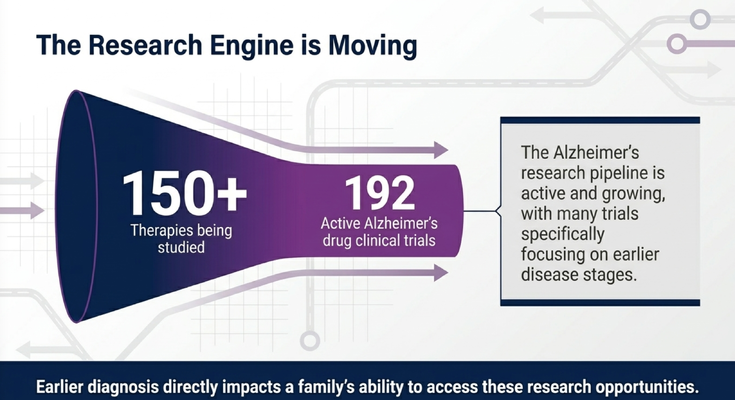
There are more than 150 therapies being studied and close to 200 active Alzheimer’s drug clinical trials. Not all of these will become approved treatments. That is not how research works. But the pipeline is active, and many trials are focused on earlier disease stages.
So when families ask, “Why should we know earlier?” the answer is not just curiosity.
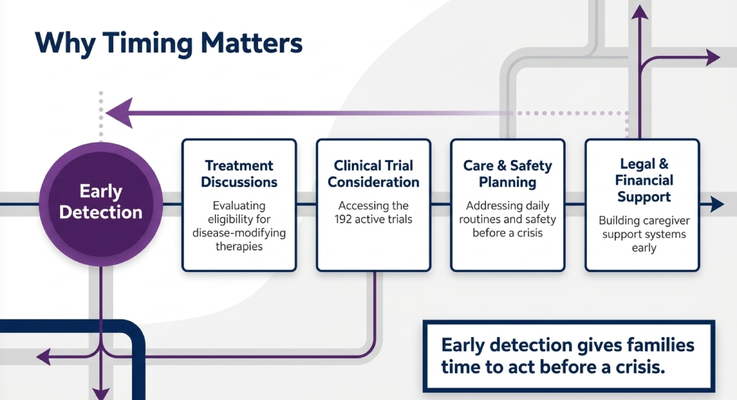
Earlier diagnosis may affect whether the person can have treatment conversations. It may affect whether they can consider clinical trials. It may affect whether the family can plan legal, financial, and safety decisions while the person can still participate.
That is the difference between being proactive and being reactive.
And in dementia care, reactive care usually costs families more emotionally, physically, and financially.
WHY TIMING MATTERS FOR FAMILIES
Early detection is not only about medications.
I want families to understand that clearly.
Early detection gives you time.
Time to talk about treatment options with qualified clinicians. Time to ask whether clinical trials are appropriate. Time to address care and safety planning before there is a crisis. Time to talk about driving before there is an accident. Time to talk about the home before the person is unsafe. Time to talk about who will make decisions before the person can no longer communicate what they want.
These conversations are not easy.
Nobody wants to sit down with their family and talk about power of attorney, healthcare proxy, living will, resuscitation preferences, finances, driving, supervision, or future care needs.
But I say this all the time:
It is better to have difficult conversations than to be in difficult situations.
Because when families wait too long, the questions become much harder.
What would Dad have wanted?
Should Mom still be driving?
Who is in charge of the finances?
Who is the healthcare proxy?
Should we move her?
Should we bring in help?
Why didn’t we talk about this earlier?
And when those questions happen during crisis, families often start fighting. Siblings disagree. Spouses feel guilty. Adult children feel trapped. The caregiver carries the burden of decisions that could have been discussed earlier.
Early detection gives families time to act before crisis makes the decisions for them.
OUR “MAMMOGRAM MOMENT” FOR ALZHEIMER’S
I recently came back from Washington, D.C., where I was advocating with the Alzheimer’s Association. I serve on the board of the South Florida Alzheimer’s Association®, and I was there with many other advocates speaking to lawmakers about the importance of Alzheimer’s screening and prevention.
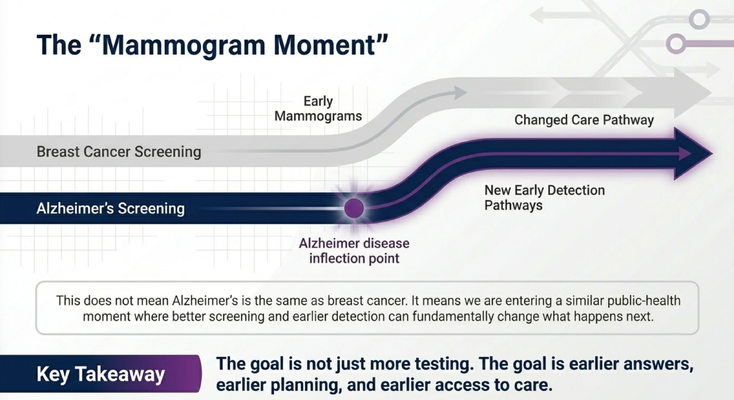
One way I explain this is what I call the “mammogram moment.”
Think about breast cancer screening.
Years ago, many cancers were found later. Then mammography changed the care pathway. Earlier screening allowed earlier detection, earlier treatment conversations, and earlier planning.
Now, let me be very clear: Alzheimer’s disease is not breast cancer. These are different diseases, different biology, different treatments, and different clinical pathways.
But the public-health lesson is similar.
When screening improves, the timing of the conversation changes.
And timing matters.
With Alzheimer’s disease, we are entering a moment where blood-based biomarker testing may help identify Alzheimer’s-related biology earlier. These tests are not meant to replace a full medical evaluation. They are not something families should use casually or interpret on their own. They are tools that need to be used with qualified clinicians as part of a broader evaluation.
But they may help close the gap between early symptoms and meaningful answers.
And for families, that gap matters.
Because the goal is not just more testing.
The goal is earlier answers, earlier planning, and earlier access to care.
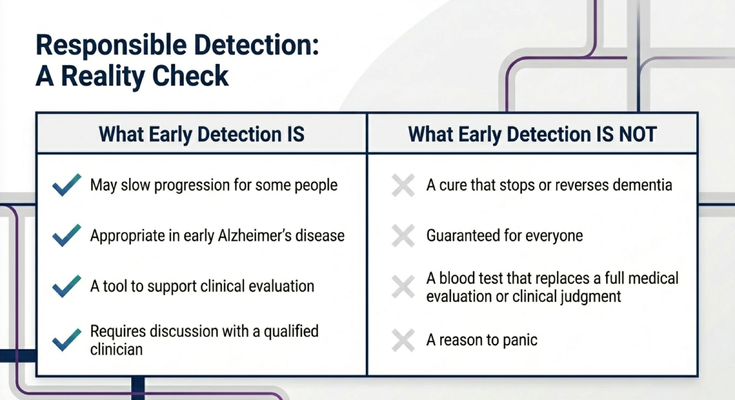
EARLY DETECTION IS NOT A CURE
Now we need to be responsible.
Early detection is important, but it is not magic.
It may help some people access earlier treatment discussions. It may support clinical decision-making. It may help families understand risk and plan sooner. It may help identify Alzheimer’s-related biology before the disease has advanced too far.
But early detection is not a cure that stops or reverses dementia.
It is not guaranteed for everyone.
It is not a blood test that replaces a physician, neurologist, cognitive evaluation, family history, functional assessment, imaging when appropriate, medication review, or clinical judgment.
And it is not a reason to panic.
That last point matters.
Because sometimes families hear “early detection” and become afraid. They think, “If we test, and something shows up, our life is over.”
No.
The point of early detection is not fear.
The point is time.
If there is a small fire, you want to know before the whole house is burning. You want the chance to act early, ask questions, gather the right team, and plan with your loved one while they still have a voice.
That is the responsible way to think about detection.
Not panic.
Preparation.
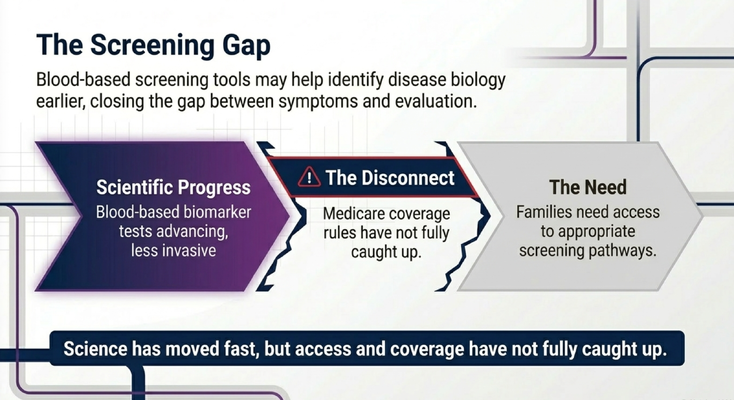
THE SCREENING GAP
Here is the problem.
Science is moving fast, but access and coverage have not fully caught up.
Blood-based biomarker tests are advancing. Some have received FDA approval or clearance. They may help clinicians identify Alzheimer’s disease biology earlier and less invasively than older pathways.
But Medicare coverage rules have not fully caught up.
And when coverage does not catch up, families feel it.
Some people may have to pay out of pocket. Some physicians may hesitate to order tests if they believe the test will not be covered. Some families may never even hear about the option. And the people who may benefit from earlier answers may stay stuck in the old model: wait until symptoms are more obvious, then react.
That is not good enough.
Families need appropriate screening pathways.
Not random testing.
Not panic testing.
Not internet interpretation.
Appropriate pathways.
That means the right patient, the right clinical context, the right provider, the right counseling, and the right follow-up plan.
Because a test without guidance can create confusion.
But a test inside a proper clinical pathway can help families move from uncertainty to action.
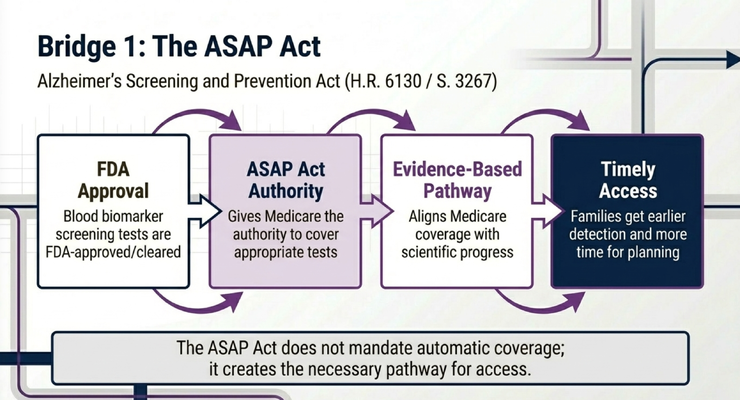
THE ASAP ACT
This is why we advocated for the ASAP Act — the Alzheimer’s Screening and Prevention Act.
The purpose is to help create a pathway for Medicare coverage of appropriate Alzheimer’s blood-based screening tests after FDA approval or clearance. The goal is to align access with scientific progress so families are not left behind simply because coverage rules have not caught up.
This does not mean automatic testing for everyone.
It does not mean every blood test should be covered without evidence.
It does not mean a blood test alone diagnoses the whole person.
It means Medicare needs the authority and pathway to cover appropriate tests when the science supports it.
That is important because policy affects real families.
Policy affects whether a doctor orders a test.
Policy affects whether a family can afford the next step.
Policy affects whether someone gets answers early enough to plan.
Policy affects whether a caregiver gets time or only gets crisis.
This is not abstract.
This is not just Washington, D.C. language.
This is about families who need answers before the disease has taken away too much.
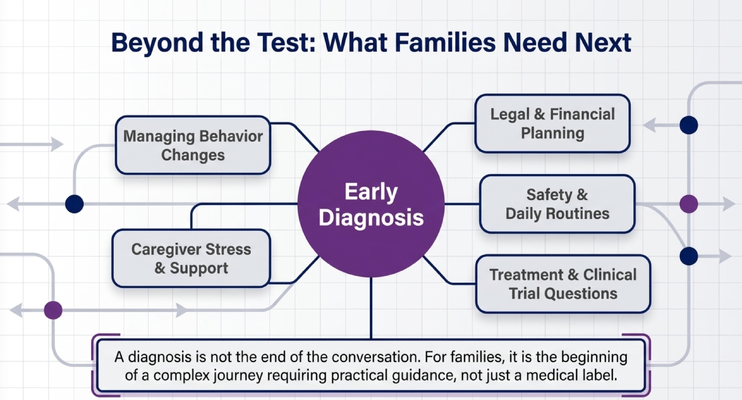
BEYOND THE TEST: WHAT FAMILIES NEED NEXT
A diagnosis is not the end of the conversation.
For families, it is the beginning of a complex journey.
This is where many families get lost.
They get a diagnosis, and then what?
What do we do about behavior changes?
What do we do when Mom sees shadows at 10 PM?
What do we do when Dad refuses to shower?
What do we do when the caregiver is exhausted?
What do we do about driving?
What do we do about the home?
What do we do about legal and financial planning?
What do we do about treatment options or clinical trials?
What do we do when the person is still early enough to participate in decisions, but nobody has told the family what questions to ask?
That is why early detection cannot stand alone.
Families need guidance after the answer.
They need help translating a diagnosis into a care plan. They need education. They need caregiver support. They need safety planning. They need help knowing when a symptom is dementia, when it may be delirium, when to call the doctor, and when the environment may be triggering the behavior.
Because families do not just need awareness.
They need access.
They need early answers.
They need trained clinicians.
They need treatment conversations.
They need a support system that helps them navigate what comes next.
THE 10 PM REALITY
Let’s make this practical.
It is 10 PM.
Mom is seeing something in the room.
She says there is a ghost.
The caregiver is scared. They do not know what is happening. Is it an infection? Is it delirium? Is it a shadow? Is it a medication issue? Is it dementia progression? Should they call 911? Should they wait? Who do they call?
This is where dementia care becomes real.
Because most families are not struggling in theory.
They are struggling inside the home.
They are struggling when the person living with dementia refuses the shower.
They are struggling when there are repeated questions all day.
They are struggling when the caregiver has no fuel left in the tank.
They are struggling when no one can come relieve them for even a few hours.
This is why early detection and caregiver support have to move together.
It is not enough to identify the disease earlier if we abandon the family afterward.
Early detection should open the door to earlier support.
Earlier education.
Earlier planning.
Earlier safety changes.
Earlier caregiver relief.
Earlier conversations with the medical team.
Earlier connection to programs that can help.
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly why the GUIDE Model matters.
GUIDE stands for Guiding an Improved Dementia Experience.
Through the GUIDE Model, eligible families may receive structured dementia-care support through MedBetter Health.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Medicare-covered respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
And I want families to understand what that means in real life.
Imagine a caregiver who can call when Mom is seeing something at night and does not know what to do.
Imagine a caregiver who needs a few hours of respite because they are exhausted and cannot keep carrying everything alone.
Imagine a family that gets help thinking through dementia behaviors, routines, safety, planning, and support.
That is what dementia care should become.
Not just a diagnosis.
Not just a pamphlet.
Not just “come back in six months.”
A real support system around the person living with dementia and the caregiver holding everything together.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia care, early Alzheimer’s detection, caregiver support, the GUIDE Model, and practical care strategies by watching Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Memory changes, Alzheimer’s screening, blood-based biomarkers, diagnosis, treatment options, clinical trial eligibility, medication decisions, caregiver burnout, safety concerns, and care planning should be discussed with qualified healthcare professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health