THE NUMBERS ARE SCREAMING
I always tell people: People talk, numbers SCREAM.
So let’s look at the numbers.
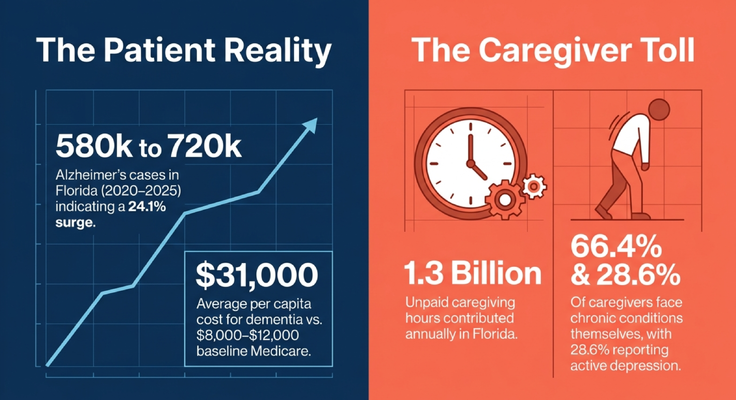
In Florida, the number of people age 65 and older living with Alzheimer’s disease was about 580,000 in 2020.
By 2025, that number was estimated to rise to 720,000.
That is a 24.1% increase in a very short period of time.
And that is only Alzheimer’s disease, not every form of dementia.
Now let me ask you something.
If we already estimate 720,000 people in Florida living with Alzheimer’s disease, but almost 40% of primary care clinicians report that they never or only sometimes feel comfortable making a dementia diagnosis, do we really think 720,000 is the full number?
Probably not.
The real number is likely higher.
And this matters because dementia is not just a diagnosis sitting in a chart. Dementia changes the cost of care, the home environment, the caregiver’s health, and the entire family system.
The average Medicare beneficiary may cost around $8,000 to $12,000 per year.
A person living with dementia may cost dramatically more.
Why?
Because dementia does not stay neatly inside one office visit.
It affects medications.
Falls.
Hospitalizations.
Behavioral symptoms.
Caregiver stress.
Emergency room visits.
Home safety.
Driving.
Sleep.
Bathing.
Nutrition.
And the family’s ability to keep the person safe at home.
THE CAREGIVER IS NOT A SIDE ISSUE
Now let’s talk about the caregiver.
In Florida, unpaid caregivers provide an enormous amount of dementia care every year. Many are spouses. Many are adult children. Many are older adults themselves.
And these caregivers are not healthy by default.
Many have chronic conditions of their own. Many experience depression. Many are sleep-deprived. Many are still working. Many are raising children. Many are quietly drowning.
My parents are caregivers for my grandmother.
My grandmother is 93 years old. My mother and father are in their 70s. They care for her every day.
Think about that.
A 70-year-old taking care of a 93-year-old.
Sleepless nights. Behavioral symptoms. Confusion. Emotional pain. Family stress. Medication questions. Safety questions.
That takes a toll.
And this is why I say something over and over again:
The caregiver is not on the side.
The caregiver is part of the care plan.
If we do not take care of the caregiver, we eventually lose the home care environment.
If the caregiver collapses, the patient is at risk.
This is the shift Medicare is trying to make through the GUIDE Model. For the first time, the system is saying, “We cannot only look at the person living with dementia. We have to look at the person caring for them too.”
That is a major paradigm shift.
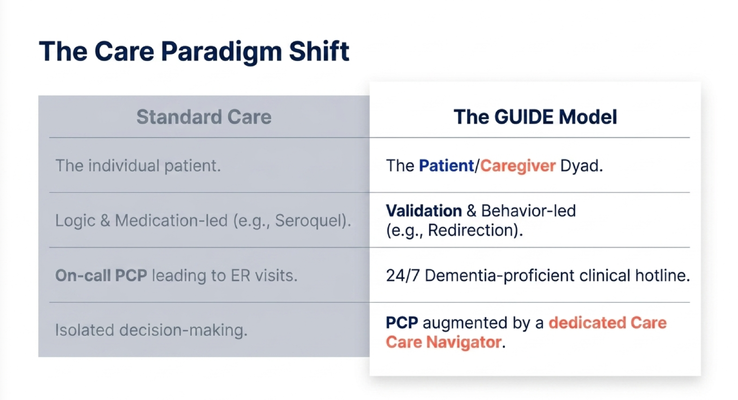
DEMENTIA CARE REQUIRES EMOTION, NOT ONLY LOGIC
As physicians, we are trained in logic.
Medication.
Diagnosis.
Guidelines.
Lab results.
Imaging.
Data.
And logic matters. Of course it matters.
But dementia care also requires emotional intelligence.
Let me give you an example from my own family.
My grandmother once asked my mother, “Where is my mother?”
Now logically, we knew the answer. Her mother had died a long time ago.
So what did my mother say?
She told the truth.
“Your mother passed away.”
And my grandmother became angry. She said something very painful to my mother, who has cared for her for years.
Those words were arrows.
So I came in and said, “Grandma, don’t worry. Your mother just went to get bread for the Sabbath. She’ll be back.”
What did I use?
Validation.
Then I redirected her. I showed her a photo album. I started naming my children. I moved her mind to another place.
And the room de-escalated.
Before learning this work more deeply, I might have used logic. I might have said, “Grandma, that is not true.”
But logic is not always the right tool when someone is living in a different reality because of dementia.
Sometimes the better tool is validation.
Sometimes it is redirection.
Sometimes it is dignity.
Sometimes it is changing the environment.
Sometimes it is understanding that the caregiver does not need more correction. They need coaching.
That is what connected dementia care has to provide.
Not just prescriptions.
A framework.
THE GUIDE MODEL: WHAT IT ACTUALLY IS
The GUIDE Model stands for Guiding an Improved Dementia Experience.
It is a Medicare dementia care model designed to support people living with dementia and the caregivers helping them at home.
MedBetterHealth.org is one of the organizations selected to participate.
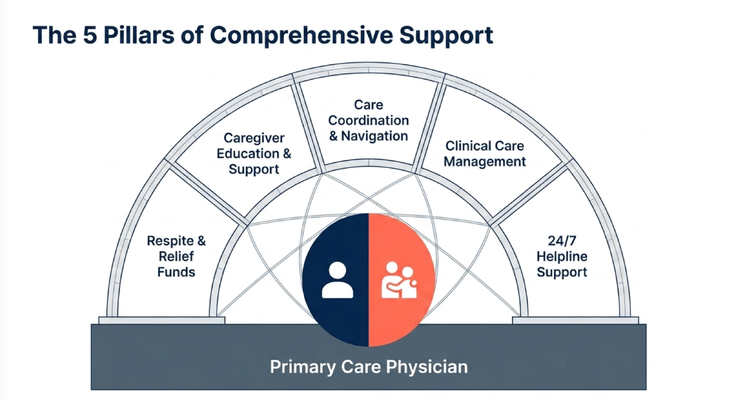
The model is voluntary. It is designed to supplement the existing care team, not replace the primary care doctor. The person’s primary care physician, specialists, pharmacy, and insurance relationships can stay in place.
That is important.
Because the point is not to take over the patient.
The point is to augment the care around the patient and caregiver.
The GUIDE Model is built around several core supports:
Care coordination and navigation.
Clinical care management.
Caregiver education and support.
Respite support.
A 24/7 helpline for non-medical dementia-related concerns.
That is the blueprint.
And when you understand what families are actually dealing with at home, you understand why each piece matters.
WHO THE GUIDE MODEL IS FOR
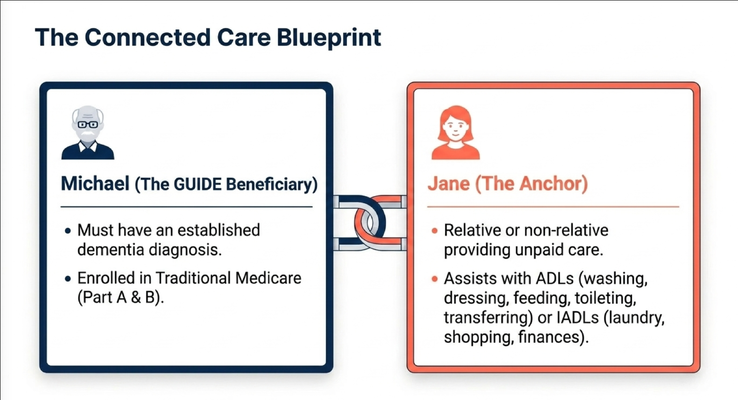
Let’s use a simple example.
Michael is the person living with dementia.
Jane is the caregiver.
For Michael to potentially qualify, he needs an established dementia diagnosis and Traditional Medicare Part A and B. The program generally does not apply if the person is enrolled in Medicare Advantage, hospice, PACE, a nursing home, or a dedicated memory care unit.
Jane is the caregiver.
She may be a relative or a non-relative, but under the GUIDE Model, she is someone providing unpaid assistance with activities of daily living or instrumental activities of daily living.
That may mean bathing, dressing, feeding, toileting, transferring, laundry, shopping, transportation, finances, appointments, or medication support.
And here is the key:
The model is not only asking, “What does Michael need?”
It is also asking, “What does Jane need in order to keep doing this safely?”
That question changes everything.
RESPITE: RELIEF FOR THE CAREGIVER
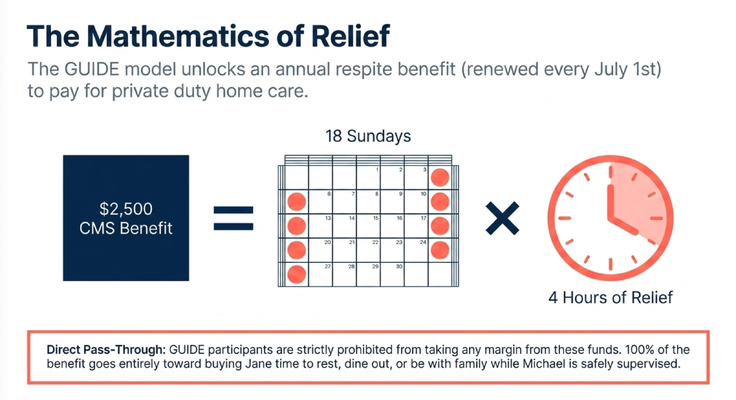
One of the most important parts of the GUIDE Model is respite.
Respite means relief for the caregiver.
Let’s say Jane is caring for Michael every day. She loves him. She wants him safe. But she is exhausted.
She cannot go out.
She cannot sleep.
She cannot go to dinner with her family.
She cannot take a break without worrying something will happen.
Respite can allow a trained private duty home care worker to come into the home so the caregiver has time to breathe.
Maybe four hours on a Sunday.
Maybe time to go to dinner.
Maybe time to go to the doctor.
Maybe time to sit with family.
Maybe time to just rest.
And some people hear the annual respite amount and say, “Dr. Erik, that is not enough to solve everything.”
Correct.
It does not solve everything.
But if you look at it correctly, those hours can be meaningful. They can give a caregiver repeated pockets of relief.
A caregiver who gets time to recover may be able to continue.
A caregiver who never gets oxygen eventually collapses.
That is why respite is not a luxury.
It is part of dementia care.
THE 10 PM CRISIS
Now let’s talk about what happens after office hours.
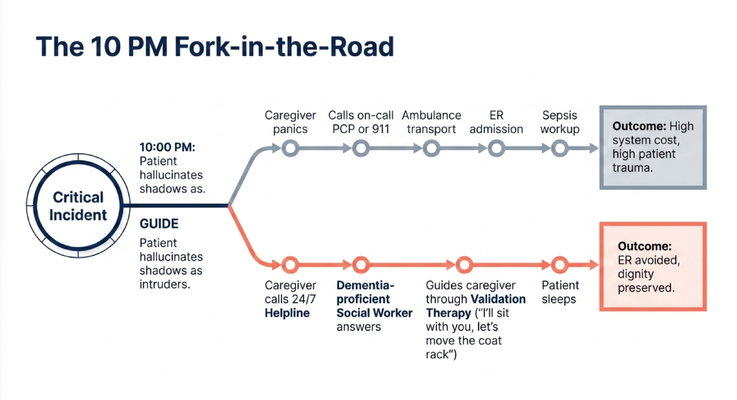
It is 10 PM.
Mom starts seeing a ghost in the room.
The caregiver says, “There is nobody there. Go back to bed. I have a big day tomorrow.”
And listen, I understand the caregiver.
They are exhausted.
They have been dealing with this all day.
They are burnt out.
But to the person living with dementia, that shadow may feel completely real.
So if you argue, correct, or dismiss it, you may escalate the fear.
A dementia-proficient support team can coach the caregiver differently.
Maybe the issue is a coat rack creating a shadow.
Maybe the blinds need to be closed earlier.
Maybe a motion-sensor night light is needed.
Maybe the right response is:
“Oh, I see it. I’ll take care of it. You stay here.”
Then remove the coat rack, sit with her, and gently say, “Mom, maybe we should keep this outside so your jackets have a place to go.”
Validation.
Redirection.
Control.
Dignity.
That can prevent an unnecessary panic, an unnecessary ER visit, and a night of trauma for everyone.
This is exactly why a 24/7 dementia helpline matters.
Dementia crises do not wait for office hours.
DECODING BEHAVIOR INSTEAD OF OVER-PRESCRIBING
Here is another example.
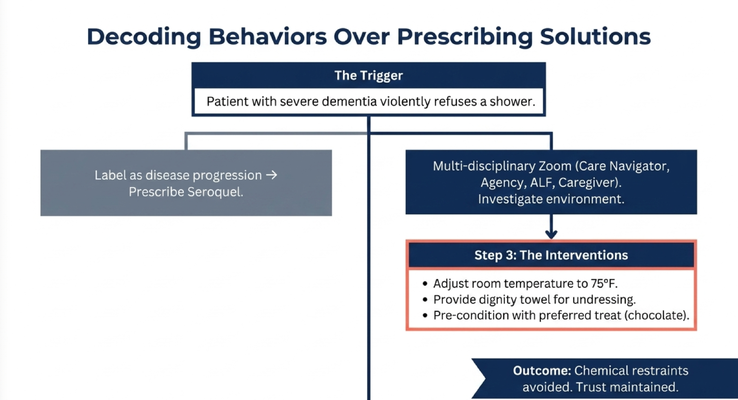
A caregiver calls and says, “My husband is in assisted living and he refuses to take a shower.”
The easy answer is to label it as dementia progression.
The easy answer is to say, “He is agitated. Increase the medication.”
But that is not where we should start.
First, we ask: what stage of dementia is he in?
Mild refusal is different from moderate refusal. Moderate refusal is different from severe refusal.
Then we ask: what is actually happening?
In this case, the person had severe dementia. But when he became soiled, he could still get up, hold the bar in the bathroom, and allow staff to clean him.
That told us something important.
He could comprehend some parts of care.
So the question became: what is different about the shower?
Maybe the room is too cold.
Maybe he feels embarrassed being undressed.
Maybe his son is present and that affects dignity.
Maybe the water temperature is uncomfortable.
Maybe the sound of water is frightening.
Maybe the approach is rushed.
So we got on a Zoom call with the caregiver, the care navigator, the private duty agency, and the care team.
Some people may say, “You spent 45 minutes talking about how to get someone to shower?”
Yes.
Because that is what mattered most to the caregiver at that moment.
We created a plan.
Warm the room.
Steam up the shower.
Preserve dignity with towels.
Use the right water temperature.
Go slowly.
Ask for comfort.
Use a preferred treat like chocolate to create a positive association.
And the caregiver called back and said it worked.
That is dementia care.
Not automatically increasing medication.
Understanding the behavior.
Protecting dignity.
Solving the actual problem.
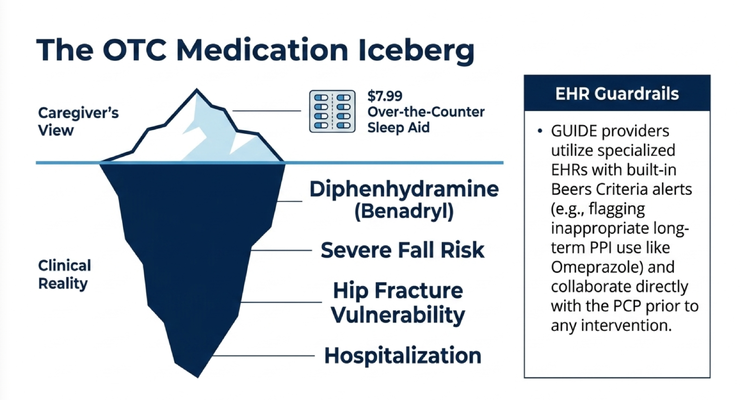
THE MEDICATION ICEBERG
Another issue we see constantly is medication risk.
A caregiver may say, “Mom only takes something over the counter for sleep.”
And when we ask to see the box, it turns out it contains diphenhydramine — Benadryl.
Now to the caregiver, it looks harmless.
It is over the counter.
It costs a few dollars.
It says sleep aid.
But for an older adult living with dementia, that medication can create serious risk: confusion, falls, dizziness, sedation, and potentially hospitalization.
This is why medication review matters.
The caregiver does not always know that an over-the-counter medication can be dangerous.
And honestly, busy primary care clinicians are managing so much already: atrial fibrillation, diabetes, high cholesterol, stroke, hospital follow-ups, 19 medications, family questions.
So GUIDE providers should not replace the primary care doctor.
They should help.
They should review the dementia-specific care picture, identify risks, flag concerns, and communicate with the PCP before making recommendations.
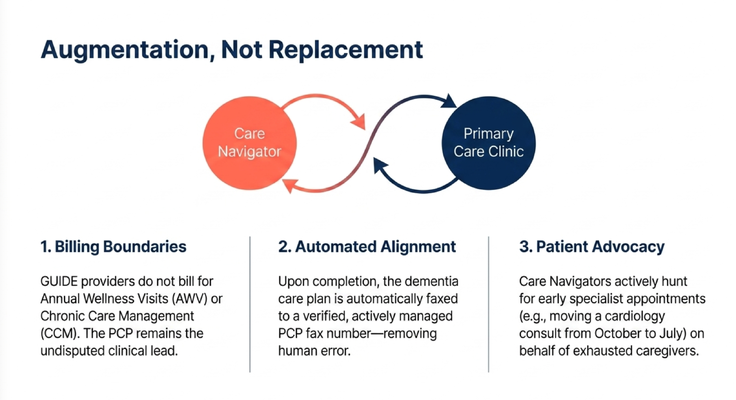
This is augmentation, not replacement.
AUGMENTATION, NOT REPLACEMENT
This is very important for professionals to understand.
The GUIDE Model is not designed to replace the primary care physician.
The PCP remains the clinical lead.
The GUIDE team supports the dementia-specific part of the picture.
For example, the care navigator may help schedule appointments, connect the caregiver to community resources, arrange transportation, follow up monthly, and help the family understand what comes next.
But the phone call itself is not the point.
The point is whether the caregiver leaves that call with something useful.
Maybe the care navigator reminds the caregiver to discuss advance directives while the loved one can still participate.
Maybe they help the family understand a medication concern.
Maybe they coordinate with the PCP.
Maybe they help the caregiver think through respite.
Maybe they help identify that the person is worsening and needs evaluation.
That is meaningful.
That is care navigation.
Not checking a box.
Adding value.
THE ACTIVATION PATHWAY
Families and professionals often ask, “How does enrollment work?”
The process is structured.
First, the GUIDE participant checks Medicare eligibility.
Then the dementia diagnosis has to be confirmed.
Then the caregiver assessment happens.
Then the patient and caregiver assessment happens with a dementia-proficient provider, including staging.
Then the data is submitted for CMS review.
This takes work because the model requires real information.
We need to understand the patient.
We need to understand the caregiver.
We need to understand the stage.
We need to understand the burden.
We need to understand what supports are needed.
This is not just a quick form.
It is an attempt to build a care plan around the real home situation.

WHAT THIS MEANS FOR FAMILIES
If you are a caregiver, here is what I want you to take away.
You should not have to do this alone.
You should not have to figure out dementia behaviors alone.
You should not have to manage medication concerns alone.
You should not have to interpret discharge paperwork alone.
You should not have to sacrifice your entire health until you become the next patient.
And you should not have to wait until crisis to get support.
Dementia care is changing.
Slowly, but it is changing.
We are moving from a model that treats the individual patient in isolation to a model that recognizes the patient and caregiver as a connected unit.
Because in dementia care, the caregiver is not extra.
The caregiver is the anchor.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about the GUIDE Model, caregiver support, respite, care navigation, behavioral symptoms, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Dementia diagnosis, medication changes, behavioral symptoms, care planning, respite, hospice, Medicare eligibility, and safety concerns should be discussed with qualified healthcare professionals.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health