
THE COLLISION OF INDEPENDENCE AND COGNITIVE DECLINE
I want to start with something very direct.
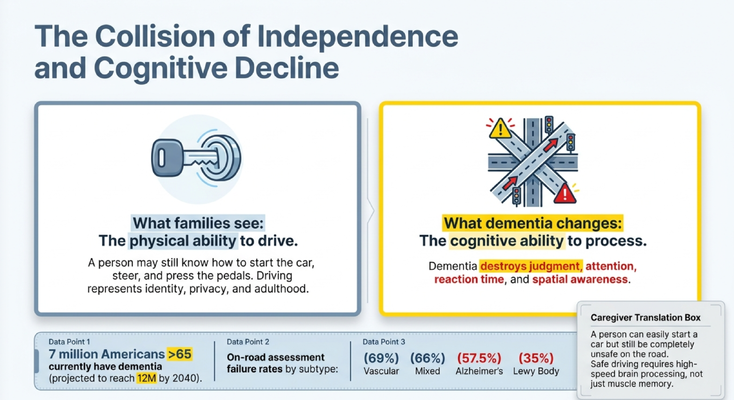
Families often see the physical ability to drive.
They see that Dad can still walk to the car. He can still start the engine. He can still press the gas. He knows where the pedals are. He has been driving for 50 years.
So the family says, “He looks fine.”
But dementia does not usually take away the physical motions of driving first.
It attacks the cognitive skills behind driving.
Judgment. Attention. Reaction time. Spatial awareness. Executive function. Insight. The ability to process multiple moving objects at once.
That is what driving requires.
A person can still know how to turn the key, but no longer have the processing speed to respond to a car braking suddenly in front of them. They may still remember the route to the grocery store, but no longer manage complex traffic, lane changes, or unexpected detours. They may still believe they are safe, but the disease may have damaged their ability to accurately judge their own impairment.
This is why driving in dementia is so difficult.
The outside can look normal while the inside processing system is failing.
DRIVING IS NOT ONE SKILL
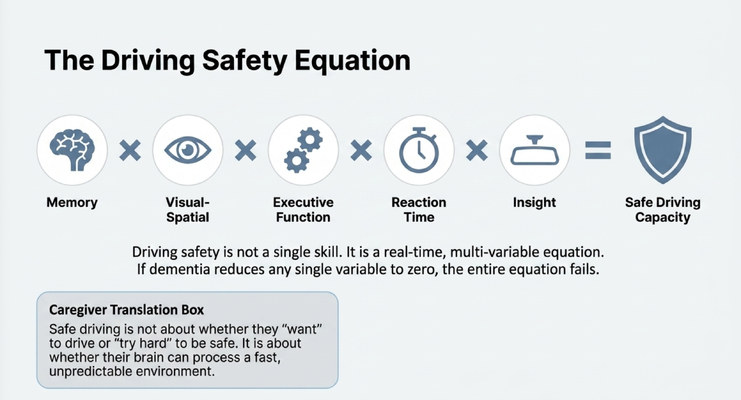
Safe driving is not one ability.
It is a real-time equation.
Memory. Visual-spatial processing. Executive function. Reaction time. Insight.
All of these have to work together.
Memory helps the person understand where they are going and recognize familiar routes. Visual-spatial processing helps them judge lanes, distance, turns, parking, and where other cars are in relation to them. Executive function helps them multitask — mirrors, speed, road signs, pedestrians, brake lights, and navigation all at the same time. Reaction time helps them respond quickly when something changes. Insight helps them recognize when they are not safe.
If dementia reduces one of those skills severely enough, the entire equation can fail.
And that is the key point.
Driving is not about trying harder.
It is about whether the brain can process the road fast enough.
A caregiver may say, “Dad promises he will be careful.” I understand that. But careful is not enough if the brain cannot process quickly. The road does not slow down because someone has dementia. Traffic does not become simpler. A child crossing the street does not give extra warning.
That is why we cannot evaluate driving safety only by intention.
We have to evaluate capacity.
WHY YOUR LOVED ONE MAY NOT SEE THE PROBLEM
One of the most frustrating parts of this conversation is that the person living with dementia may truly believe they are fine.
You may say, “Dad, I don’t think it is safe for you to drive.”
And Dad says, “What are you talking about? I drive fine.”
You may say, “Mom, you got lost twice this month.”
And Mom says, “That happens to everyone.”
You may point to dents on the car, tickets, missed stop signs, or confusion, and the person still does not seem to understand the seriousness of it.
There is a word caregivers need to know: anosognosia.
Anosognosia means the person may genuinely be unable to recognize their own impairment because of changes in the brain.
This is not always denial.
This is not always stubbornness.
This is not always pride.
Sometimes, the disease has damaged the person’s ability to self-check. In their reality, they are still driving fine. They are not lying to you. They are not trying to manipulate you. They may truly believe what they are saying.
That does not make the risk less real.
But it should change how we approach the conversation.
If the person cannot recognize the impairment, arguing harder usually will not work. You may win the facts and lose the relationship. You may prove your point and still not get cooperation.
So the goal is not to shame them.
The goal is to move the decision away from a family argument and toward an objective safety process.
THE RED FLAG FILTER
So how do families know when to act?
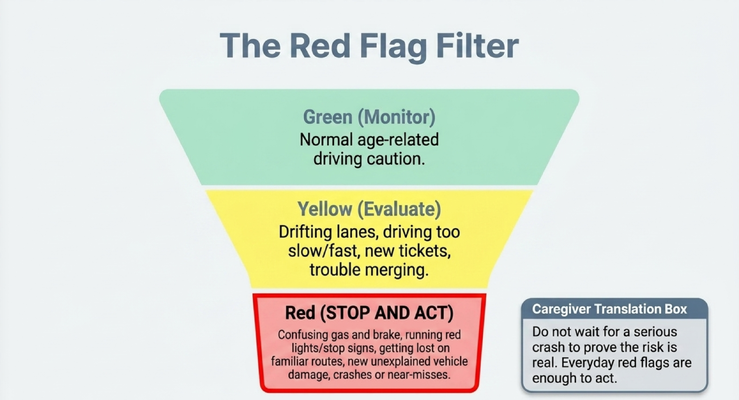
I want you to think in three categories: green, yellow, and red.
Green means monitor. This is normal age-related caution. There are no incidents. The caregiver has no major concerns. In this stage, you start the conversation early. You do not wait for a crisis. You begin discussing what the plan will be if driving ever becomes unsafe.
Yellow means evaluate. This is when you start seeing warning signs: drifting lanes, driving too slowly, getting new tickets, trouble merging, discomfort in complex traffic, or mild confusion in unfamiliar areas.
Yellow does not mean panic.
But yellow does mean you should talk to the doctor and consider a formal driving evaluation.
Red means stop and act.
Confusing the gas and brake. Running red lights. Missing stop signs. New unexplained vehicle damage. Getting lost on familiar routes. Crashes. Near misses.
Do not wait for a serious crash to prove the risk is real.
Everyday red flags are enough to act.
This is one of those areas where families cannot afford to say, “Let’s just see what happens.” Because what happens may be irreversible.
THE DRIVING DECISION MATRIX
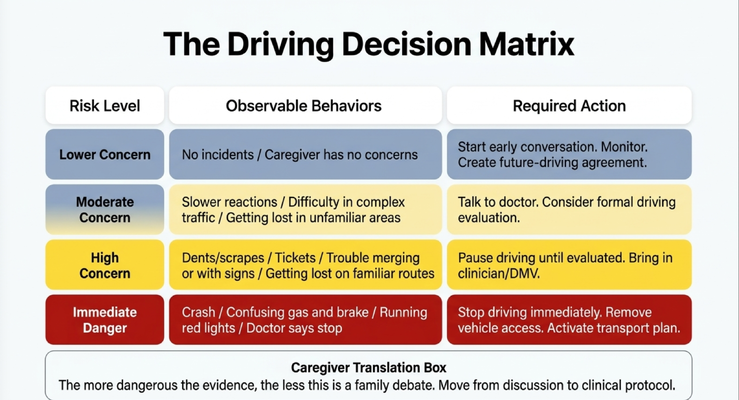
The more dangerous the evidence, the less this is a family debate.
That is the sentence I want you to remember.
If there are no incidents and no caregiver concerns, start the conversation early and monitor. Create a future-driving agreement before emotions are high.
If there are moderate concerns — slower reactions, trouble in complex traffic, getting lost in unfamiliar areas — talk to the doctor and consider a formal driving evaluation.
If there are high concerns — dents, scrapes, tickets, trouble merging, trouble with signs, getting lost on familiar routes — pause driving until the person is evaluated. Bring in the clinician. Bring in the DMV process if needed. Do not let this stay only between you and your loved one.
If there is immediate danger — a crash, gas and brake confusion, running red lights, a doctor saying stop — driving should stop immediately. Vehicle access may need to be removed, and a transportation plan needs to be activated.
I know this sounds harsh.
But sometimes love has to make the hard decision before tragedy makes it for you.
And I want to be clear: the caregiver does not have to be the evaluator. You are not the driving test. You are not the DMV. You are not the occupational therapist.
You are the person seeing the red flags.
Your job is to bring the concern into a clinical process.
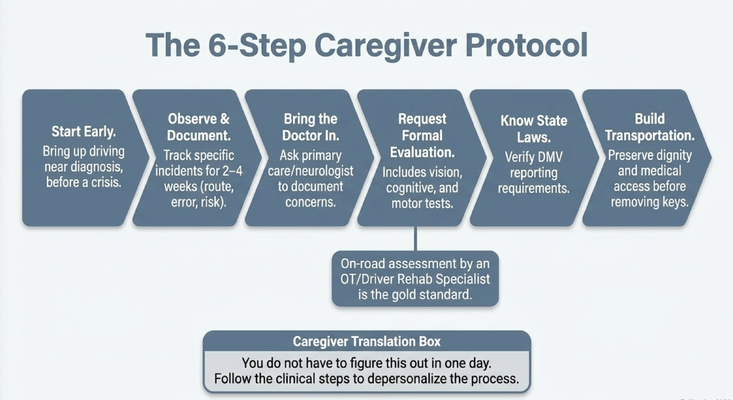
THE 6-STEP CAREGIVER PROTOCOL
So what should families actually do?
First, start early. Do not wait until there is a crash. Bring up driving before the crisis. Ask questions like, “Dad, if there ever comes a time when driving is not safe, how would you want us to handle it?”
Second, observe and document. Do not rely only on feelings. Write down specific incidents: dates, routes, tickets, dents, near misses, getting lost, confusion, wrong turns, or calls for help.
Third, bring the doctor in. Ask the primary care doctor, neurologist, or care team to document the concerns. The caregiver should not carry this alone as a family opinion.
Fourth, request a formal driving evaluation. The gold standard is often an on-road assessment by an occupational therapist or driver rehabilitation specialist, along with cognitive, vision, and motor testing.
Fifth, know your state laws. Reporting rules vary by state. Do not assume the rules are the same everywhere. Some states have mandatory physician reporting. Others rely more on self-reporting or voluntary reporting.
Sixth, build transportation before removing the keys. This is critical. If you take away driving without replacing the transportation function, you may create isolation, anger, missed appointments, loss of dignity, and caregiver overload.
The goal is not just to remove the car.
The goal is to replace the system the car provided.
HOW TO HAVE THE CONVERSATION
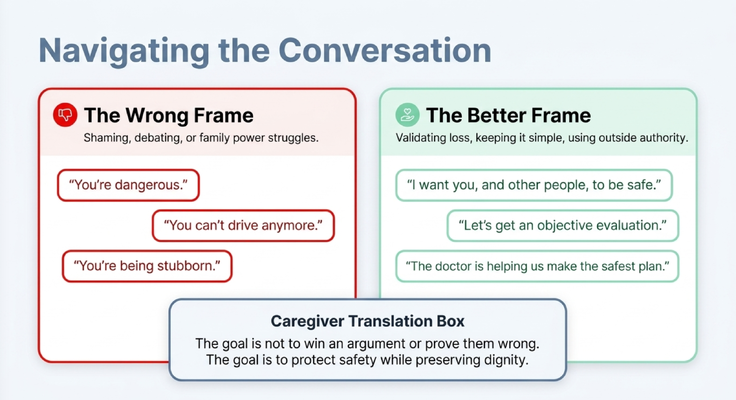
The way you say it matters.
The wrong frame sounds like this:
“You’re dangerous.”
“You can’t drive anymore.”
“You’re being stubborn.”
I understand why caregivers say things like this. They are scared. They are exhausted. They are trying to prevent something terrible from happening.
But this usually does not work.
Remember, anosognosia may be involved. The person may not be able to see what you see. So when you say, “You’re dangerous,” they may hear an insult. When you say, “You can’t drive,” they may hear control. When you say, “You’re being stubborn,” they may feel attacked.
A better frame is simple and respectful:
“I want you and other people to be safe.”
“Let’s get an objective evaluation.”
“The doctor is helping us make the safest plan.”
This moves the conversation away from shame and toward safety.
It also uses outside authority. Not as a weapon, but as a support. The caregiver should not have to be the bad guy. The family should not have to turn this into a personal battle.
The goal is not to win an argument or prove the person wrong.
The goal is to protect safety while preserving dignity.
THE HIDDEN SHIFT IN CAREGIVER LABOR
There is another part of this conversation that families do not always prepare for.
When the person living with dementia stops driving, the caregiver often becomes the transportation system.
Doctor visits. Grocery shopping. Pharmacy pickups. Social visits. Adult day care. Emergencies. Family events. Lab appointments. Specialist visits.
That is a major shift in caregiver labor.
And if we do not talk about it honestly, we make the caregiver feel guilty for struggling.
The driving decision is not only a patient safety issue. It is also a caregiver workload issue.
If Dad stops driving, who takes him to the doctor? Who gets the groceries? Who picks up medication? Who brings him to adult day care? Who handles the emergency call when something changes? Who manages the calendar?
These questions matter.
Because if we remove driving but do not build a support system, we may protect against one risk while creating another crisis.
This is why planning has to include transportation, home care support, community programs, family schedules, delivery services, telehealth when appropriate, and care navigation.
Do not just ask, “Should Mom stop driving?”
Ask, “What system replaces driving when she does?”
THE ETHICAL BALANCE
This is one of the hardest ethical decisions in dementia care.
On one side, there is public safety, family liability, and cognitive decline.
On the other side, there is autonomy, dignity, independence, and identity.
Both sides matter.
If you only focus on safety, you may strip away dignity. If you only focus on independence, you may ignore serious risk.
So how do we balance it?
We build a transportation plan.
That is the bridge.
You are not just removing a car. You are replacing transportation. You are replacing access. You are replacing independence in a safer form.
That may mean family rides. Ride-share when appropriate. Paratransit. Senior transportation. Adult day programs. Pharmacy delivery. Grocery delivery. Care navigation. Telehealth. Home visits. Community support.
This is how we protect the body without breaking the spirit.
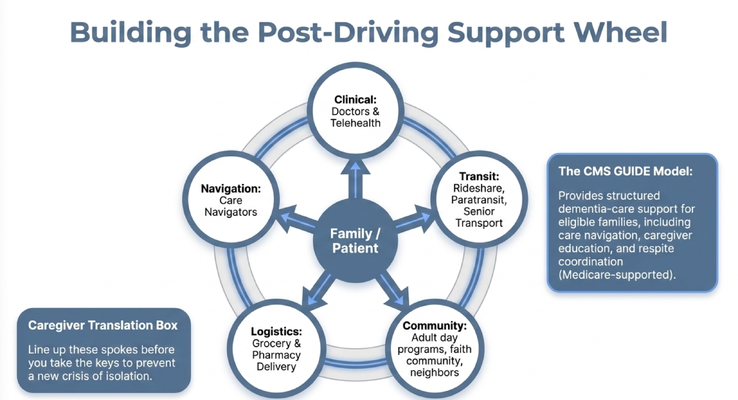
THE GUIDE MODEL: MEDICARE’S NEW DEMENTIA CARE PROGRAM
This is exactly the type of decision caregivers should not have to navigate alone.
Driving and dementia is not just a medical issue. It is a safety issue, a dignity issue, a transportation issue, a caregiver burden issue, and often a family conflict issue.
That is why Medicare created the GUIDE Model — Guiding an Improved Dementia Experience.
MedBetter Health is proud to participate in this 8-year CMS initiative designed to support people living with dementia and the family caregivers caring for them at home.
Through the program, eligible beneficiaries and caregivers may receive:
A dedicated Care Navigator who coordinates dementia care and support
A 24/7 helpline for behavioral and non-medical dementia-related concerns
Respite care support so caregivers can rest and recover
Personalized dementia care plans and caregiver education
Ongoing support navigating the realities of dementia care at home
In a situation like driving, this kind of support matters.
A caregiver may need help figuring out who can evaluate driving safety. They may need help talking to the doctor. They may need help documenting concerns. They may need help building a transportation plan. They may need help managing the emotional fallout when a loved one feels angry, embarrassed, or betrayed.
This is the kind of problem that does not get solved in a five-minute office visit.
Families need guidance.
They need a process.
They need someone to help them think through the next step.
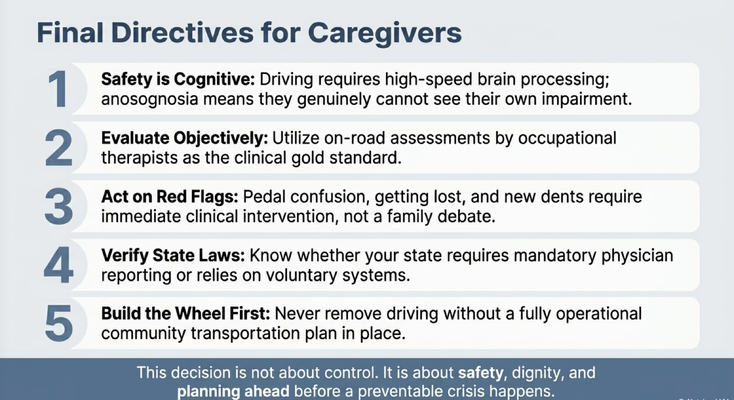
THE FINAL DIRECTIVES FOR CAREGIVERS
If you are dealing with driving concerns in your family, here is what I want you to remember.
Safety is cognitive. Driving requires high-speed brain processing, not just physical ability.
Evaluate objectively. Use clinicians and formal driving assessments instead of turning this into a family argument.
Act on red flags. Pedal confusion, getting lost, new dents, tickets, near misses, and running lights require action.
Verify state laws. Reporting rules vary. Know the requirements in your state before acting.
Build the wheel first. Never remove driving without creating a real transportation plan.
This decision is not about control.
It is about safety, dignity, and planning ahead before a preventable crisis happens.
THE NEXT STEP FOR YOUR FAMILY
If you are caring for someone living with dementia in Florida or New York, MedBetter Health may be able to support your family through the GUIDE Model.
You can check eligibility here:
https://medbetterhealth.org/guide
MedBetter Health currently serves eligible families in Florida and New York only.
Even if you are not eligible for the GUIDE Model, MedBetter Health remains committed to supporting caregivers with practical, evidence-based dementia education.
Straight Talk With Dr. Erik

Learn more about dementia driving safety, caregiver decision-making, and practical dementia care by watching the full video and subscribing to Straight Talk with Dr. Erik.
https://www.youtube.com/@ErikIlyayev
This is education, not medical advice. Driving laws, reporting requirements, and medical recommendations vary by state and by individual situation. If you are concerned about dementia and driving safety, speak with a qualified healthcare professional and check your state’s DMV requirements.
Thank you for reading The Dementia Times.
With gratitude,
Dr. Erik Ilyayev, MD
CEO, MedBetter Health